GH Peptides for Muscle: Hype vs Evidence
Visceral Fat and Growth Hormone
2.1 kg lean mass gain
Systematic reviews find growth hormone increases lean body mass by roughly 2 kg, but strength and exercise capacity do not improve.
Sigalos & Pastuszak, Sexual Medicine Reviews, 2018
Sigalos & Pastuszak, Sexual Medicine Reviews, 2018
If you only read one thing
Growth hormone peptides raise your GH and IGF-1 levels — that part is real. But they mostly don't build actual muscle. When studies measure body composition, the 1–2 kg of 'lean mass' that shows up on the scan is largely water, connective tissue, and glycogen — not new muscle fiber. Strength and exercise performance don't improve. No controlled human trial has tested CJC-1295, ipamorelin, or GHRP-6 for muscle outcomes. The clearest benefit is preventing muscle loss during dieting or illness, not building new muscle in healthy, training people.
Growth hormone peptides are among the most popular compounds in the peptide space, marketed with claims of muscle growth, fat loss, and body recomposition. Peptides like CJC-1295, ipamorelin, GHRP-6, and the oral secretagogue MK-677 (ibutamoren) all reliably increase circulating growth hormone and IGF-1 levels. That hormonal effect is well-documented across multiple clinical trials.[1] The question is whether those hormone changes translate into the muscle growth that users expect. For the broader relationship between growth hormone, body composition, and visceral fat, the evidence tells a more complex story than the marketing suggests.
The short answer: growth hormone and its secretagogues increase lean body mass on a scale. They do not reliably increase muscle protein synthesis, muscle strength, or exercise performance in healthy adults. The lean mass gains are largely explained by water retention, not new muscle tissue.
Key Takeaways
- Growth hormone peptides raise your GH levels — that part works. Whether they build real muscle is a very different question.
- The 2 kg of "lean mass" that shows up on body scans is mostly water, connective tissue, and glycogen — not new muscle fiber.
- Strength and exercise performance don't improve, even when the scale says you gained lean mass.
- The two most popular muscle-building peptides, CJC-1295 and ipamorelin, have zero human trials measuring muscle outcomes.
- MK-677 reliably raises blood sugar in every trial long enough to measure it — a clear trade-off for unclear gains.
- Where these peptides actually shine is preventing muscle loss during a hard diet or illness, not building new muscle.
- Testosterone tells muscle fibers to grow. GH mostly tells your body to hold more fluid. They're not interchangeable.
Evidence Matrix
What Has Actually Been Tested
Most GH peptides have hormone data but zero muscle outcome trials
| Peptide | GH/IGF-1 data | Body comp trial | Strength data | Human RCT |
|---|---|---|---|---|
| MK-677Oral | ✓ | ✓ | ✗ | ✓ |
| TesamorelinInjection | ✓ | ✓ | ✗ | ✓ |
| CJC-1295Injection | ✓ | ✗ | ✗ | ✗ |
| IpamorelinInjection | ✓ | ✗ | ✗ | ✗ |
| GHRP-6Injection | ✓ | ✗ | ✗ | ✗ |
MK-677: Fat-free mass ↑ but glucose impaired
Tesamorelin: FDA-approved; +1.42 kg lean mass in HIV patients
CJC-1295: GH 2-10× rise, but zero outcome studies
Ipamorelin: Clean GH release (no cortisol), but no body comp data
GHRP-6: Raises GH + cortisol + appetite; zero outcome data
Source: Sigalos & Pastuszak (2018); Teichman (2006); Svensson (1998); Raun (1998); Badran (2026)
The Hormone-to-Muscle Gap
Growth hormone secretagogues work. They raise GH and IGF-1 levels. This is not in dispute. CJC-1295, a long-acting GHRH analog, produced dose-dependent GH increases of 2- to 10-fold that persisted for 6 or more days after a single injection, with IGF-1 elevations lasting 9-11 days.[2] MK-677, taken orally at 25 mg daily, increased IGF-1 by approximately 40% in obese men over 8 weeks.[3] These are real, measurable hormonal effects.
The problem is the logical leap from "raises GH" to "builds muscle." Multiple systematic reviews of exogenous GH administration (which produces far higher GH levels than any secretagogue) have found a consistent pattern: lean body mass increases by roughly 2 kg, but muscle protein synthesis rates, muscle strength, and exercise capacity do not change.[1] Meta-analyses of RCTs confirm that GH increases total water content and extracellular water without changing muscle protein synthesis rates. The gains on body composition scans are driven by fluid retention, not contractile tissue.
This means the "lean mass" gains measured by DEXA or bioimpedance are predominantly water, not contractile muscle tissue. GH increases extracellular fluid volume, connective tissue hydration, and glycogen storage, all of which register as lean mass on body composition scans but do not produce the functional muscle gains that users seek.
What the DEXA Scan Is Really Measuring
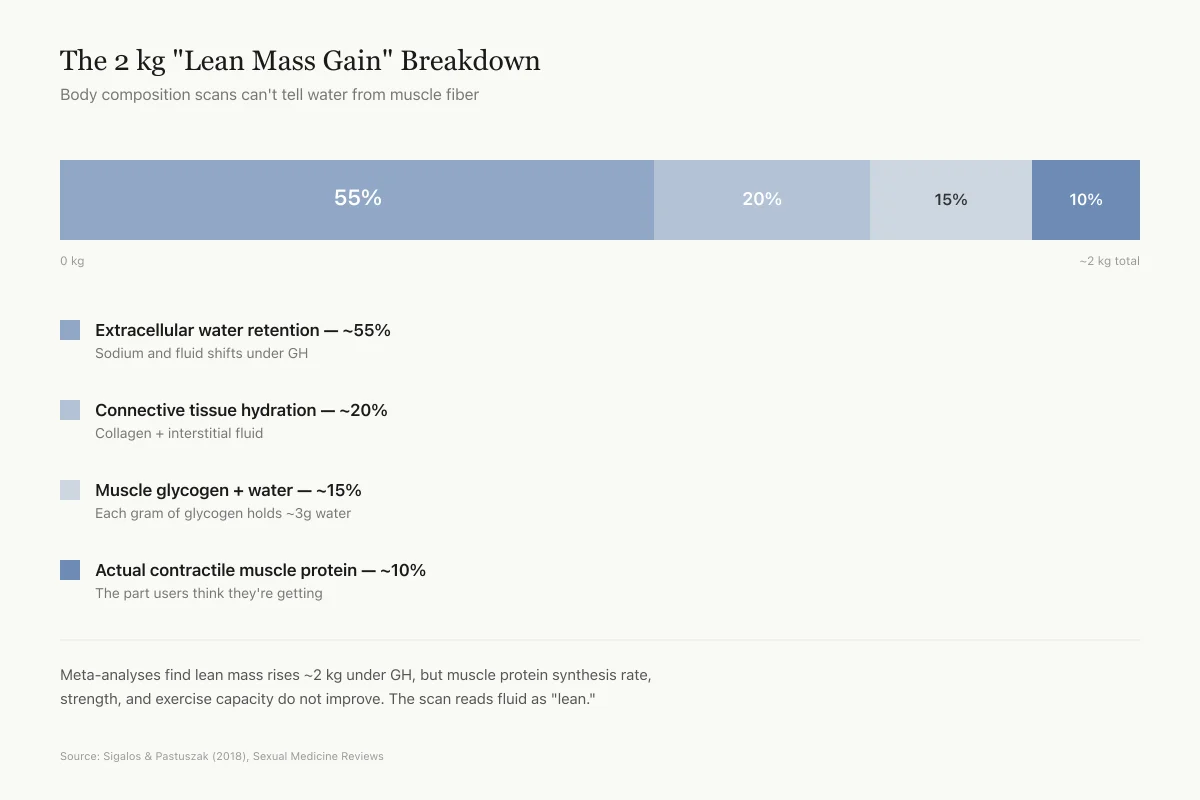
The 2 kg "Lean Mass Gain" Breakdown
Body composition scans can't tell water from muscle fiber
Sodium and fluid shifts under GH
Collagen + interstitial fluid
Each gram of glycogen holds ~3g water
The part users think they're getting
Meta-analyses find lean mass rises ~2 kg under GH, but muscle protein synthesis rate, strength, and exercise capacity do not improve. The scan reads fluid as "lean," so the number looks like muscle growth when it mostly isn't.
Source: Sigalos & Pastuszak (2018), Sexual Medicine Reviews — synthesis of GH body composition literature
 View as image
View as imageWhat MK-677 Actually Does to Body Composition
MK-677 (ibutamoren) has the most body composition data of any GH secretagogue because it is orally active and was developed through formal pharmaceutical trials.
Svensson et al. (1998) randomized 24 obese men to MK-677 25 mg or placebo daily for 8 weeks.[3] Fat-free mass increased by DEXA (P less than 0.01) and by a four-compartment model (P less than 0.05). IGF-1 rose approximately 40%. Basal metabolic rate increased at 2 weeks but was no longer significant at 8 weeks. Total and visceral fat were not significantly changed. The trade-off: an oral glucose tolerance test showed impaired glucose homeostasis at both 2 and 8 weeks. This insulin resistance signal has appeared in every MK-677 trial of meaningful duration.
In a separate trial, Murphy et al. (1998) used MK-677 to reverse diet-induced nitrogen wasting in 8 healthy men on caloric restriction.[4] During 7 days of MK-677, mean daily nitrogen balance shifted from -1.48 g/day with placebo to +0.31 g/day (P less than 0.01). This nitrogen-sparing effect is real and clinically relevant for catabolic states (surgery recovery, prolonged bed rest, severe caloric deficit). It does not, however, demonstrate muscle building in fed, training individuals. Nitrogen balance is a surrogate measure that can be influenced by water shifts, and this trial did not measure muscle mass, strength, or protein synthesis directly.
The distinction matters: MK-677 may protect against muscle loss during caloric restriction. That is a different claim than "builds muscle," and the evidence supports the former far more than the latter. For more on MK-677's metabolic trade-offs, see MK-677 and insulin resistance.
Safety
ModerateMK-677 reliably impairs blood sugar control
Concern
Every controlled MK-677 trial long enough to measure it has shown impaired glucose tolerance, reduced insulin sensitivity, or both. Fasting glucose rose by roughly 26% in one elderly trial. This effect has appeared in healthy young men, obese adults, the elderly, and Alzheimer's patients — it is not a niche finding.
What the research says
The insulin resistance appears reversible when MK-677 is stopped, and no trial has shown progression to diabetes over the time periods studied. But long-term users and anyone with pre-diabetes, insulin resistance, or a family history of type 2 diabetes are taking a clear metabolic trade-off for unclear body-composition benefits.
Particularly relevant for: Anyone using MK-677, especially with pre-existing glucose issues
What to do
Check fasting glucose and HbA1c before starting and at 4–8 weeks. Stop if either rises meaningfully. Don't combine with other compounds that impair insulin sensitivity.
Chapman (1996); Svensson (1998); Nass (2008); Sevigny (2008) — every controlled trial of meaningful duration
CJC-1295: Hormones Without Outcomes
CJC-1295 is one of the most commonly used GH peptides, yet the evidence gap is striking. The landmark Teichman et al. (2006) trial demonstrated its pharmacological activity: single subcutaneous injections in healthy adults produced sustained GH elevation for 6+ days and IGF-1 elevation for 9-11 days, with evidence of cumulative effects after multiple doses.[2] The half-life of 5.8-8.1 days makes it one of the longest-acting GHRH analogs available.
No published study has measured the effects of CJC-1295 on muscle mass, body composition, strength, exercise performance, recovery, sleep quality, or body fat in humans. The entire body of human evidence consists of pharmacokinetic and pharmacodynamic studies measuring hormone levels. Every claim about CJC-1295 building muscle is extrapolated from its hormonal effects, not from direct measurement of muscle outcomes. For more on what the CJC-1295 data actually shows, see CJC-1295 and IGF-1 elevation.
Ipamorelin: Clean GH Release, No Body Composition Data
Ipamorelin holds a unique pharmacological position among GH secretagogues. Raun et al. (1998) demonstrated that ipamorelin stimulates GH release with potency comparable to GHRP-6, but without raising ACTH or cortisol even at doses more than 200 times the ED50 for GH release.[5] This selectivity profile is genuinely distinctive. GHRP-2 and GHRP-6 both increase cortisol and ACTH, which can promote fat storage and muscle catabolism, partially counteracting the anabolic signal from GH elevation.
Ipamorelin's clean hormonal profile makes it a theoretically better candidate for muscle-building applications. But theory is not evidence. No published human study has measured ipamorelin's effects on muscle mass, body composition, strength, or exercise performance. The selectivity advantage exists at the hormonal level; whether it translates to meaningful differences in body composition remains untested. For more on ipamorelin's pharmacology, see ipamorelin: the selective GH secretagogue.
Tesamorelin: The Only FDA-Approved GHRH Analog
Tesamorelin is the only GHRH analog with FDA approval (for HIV-associated lipodystrophy) and the most robust body composition data in the GH secretagogue class. A 2026 meta-analysis of 5 randomized controlled trials found tesamorelin increased lean body mass by 1.42 kg (95% CI 1.13-1.71, P less than 0.001) while reducing visceral adipose tissue by 27.71 cm2 and trunk fat by 1.18 kg.[6]
These are the strongest body composition results for any GH secretagogue, and they come from a population with HIV-associated metabolic dysfunction, not healthy adults seeking muscle growth. Whether the lean mass gains represent true muscle hypertrophy or fluid shifts is not resolved by the available imaging data. The visceral fat reduction is more clearly established and may be the more clinically relevant finding, particularly for the fat loss evidence in this class.
Why GH Alone Doesn't Build Muscle
The biology explains the evidence gap. Growth hormone acts on muscle primarily through IGF-1, which stimulates muscle protein synthesis. But in healthy, fed adults with normal GH levels, the rate-limiting step for muscle growth is mechanical tension (resistance training), not GH or IGF-1 availability. Raising GH above normal physiological levels increases fluid retention, connective tissue synthesis, and nitrogen balance but does not proportionally increase myofibrillar protein synthesis, the process that produces larger, stronger muscle fibers.
This is why athletes who use supraphysiological doses of actual recombinant HGH (at levels far exceeding what any secretagogue can produce) do not gain muscle mass comparable to anabolic steroids. GH and testosterone operate through different pathways. Testosterone directly activates the androgen receptor in muscle fibers, driving myofibrillar protein synthesis. GH primarily affects connective tissue, fluid balance, and fat metabolism. The comparison between GH secretagogues and exogenous HGH reinforces this distinction.
Mechanism Comparison
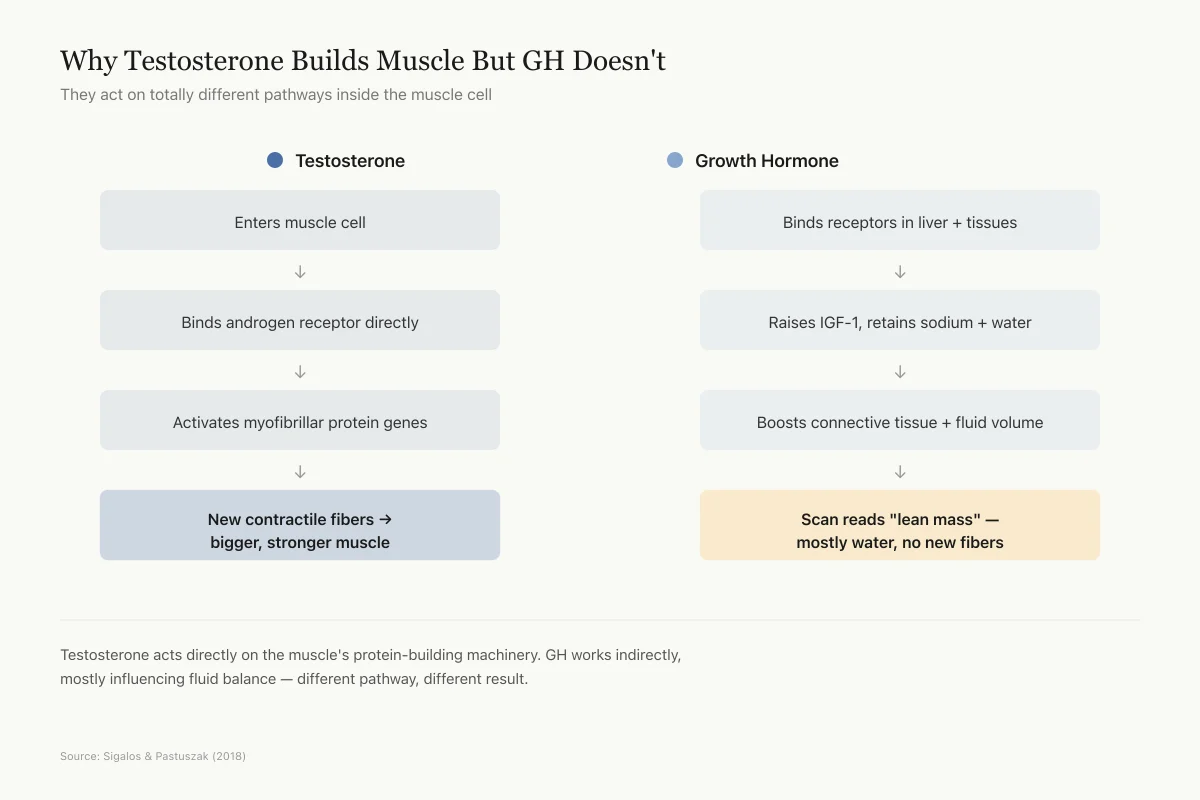
Why Testosterone Builds Muscle But GH Doesn't
They act on totally different pathways inside the muscle cell
Testosterone acts directly on the muscle fiber's protein-building machinery. GH works indirectly, mostly influencing fluid balance and connective tissue. That is why athletes on high-dose HGH don't gain the same muscle as those on anabolic steroids — different pathway, different result.
Source: Sigalos & Pastuszak (2018) — review of GH secretagogue mechanism and outcomes
 View as image
View as imageThe one context where GH-axis stimulation consistently preserves or builds lean tissue is in GH-deficient populations: elderly adults with age-related GH decline, HIV patients with wasting, and people in severe catabolic states. For these groups, restoring GH toward physiological levels can meaningfully improve body composition. For young, healthy, well-fed individuals who train regularly, the evidence for GH peptides producing meaningful muscle growth above what training alone provides is absent.
GHRP-6 and GHRP-2: The Older Peptides
GHRP-6 and GHRP-2 are earlier-generation growth hormone releasing peptides that preceded ipamorelin. Both stimulate GH release through the ghrelin receptor (GHS-R1a), but with less selectivity than ipamorelin. GHRP-6 is particularly known for increasing appetite through ghrelin pathway activation, and both GHRP-6 and GHRP-2 raise ACTH and cortisol alongside GH.[5]
The cortisol elevation is pharmacologically meaningful for muscle-building claims. Cortisol is catabolic: it promotes protein breakdown, increases fat deposition (particularly visceral), and opposes the anabolic effects of GH and IGF-1. A peptide that raises both GH and cortisol simultaneously sends competing signals to muscle tissue. This is one reason the Raun et al. selectivity data on ipamorelin generated interest: removing the cortisol component could theoretically improve the anabolic-to-catabolic ratio.
No published human trial has measured the effects of either GHRP-6 or GHRP-2 on muscle mass, strength, or body composition. The available human data consists of acute pharmacokinetic studies measuring hormone responses to single doses. Claims about muscle-building effects of these peptides rely entirely on the indirect logic of GH elevation.
The Combination Problem
Many users combine GH peptides (e.g., CJC-1295 + ipamorelin), expecting synergistic effects. No published study has tested this combination for any outcome in humans. The hormonal logic (GHRH analog + ghrelin mimetic = amplified GH pulse) is pharmacologically plausible, but the body composition outcomes remain speculative. Without controlled data, it is impossible to determine whether combination protocols produce different results from single agents, or whether they simply produce a larger hormonal spike with the same water-retention-driven lean mass changes.
The same evidence gap applies to dosing protocols. Users commonly discuss "saturation doses," cycling schedules, and timing relative to meals or training. None of these protocols have been tested in controlled settings for body composition or muscle outcomes. The pharmacokinetic data from formal trials used fixed doses on fixed schedules; any modifications to these protocols are anecdotal.
The Bottom Line
Growth hormone secretagogues reliably increase GH and IGF-1 levels in humans. The lean mass gains measured on body composition scans (1-2 kg across trials) are largely explained by water retention, not muscle fiber hypertrophy. No published RCT has tested CJC-1295, ipamorelin, or GHRP-6 for muscle-building outcomes in healthy humans. MK-677 has the most data, showing nitrogen-sparing effects during caloric restriction and fat-free mass increases in obese men, but with consistent impairment of glucose tolerance. The evidence supports GH peptides for anti-catabolic applications (preventing muscle loss during restriction or illness) far more convincingly than for anabolic applications (building muscle in healthy, training individuals).
Sources & References
- 1RPEP-03907·Sigalos, John T et al. (2018). “The Safety and Efficacy of Growth Hormone Secretagogues..” Sexual medicine reviews.Study breakdown →PubMed →↩
- 2RPEP-01190·Teichman, Sam L et al. (2006). “CJC-1295 in Humans: Single Injection Sustains GH and IGF-1 Elevation for Up to 2 Weeks.” The Journal of clinical endocrinology and metabolism.Study breakdown →PubMed →↩
- 3RPEP-00497·Svensson, J et al. (1998). “Oral MK-677 Increases Growth Hormone, Lean Mass, and Calorie Burning in Obese Men.” The Journal of clinical endocrinology and metabolism.Study breakdown →PubMed →↩
- 4RPEP-00480·Murphy, M G et al. (1998). “MK-677 Pill Reverses Muscle Breakdown From Calorie Restriction.” The Journal of clinical endocrinology and metabolism.Study breakdown →PubMed →↩
- 5RPEP-00485·Raun, K et al. (1998). “Ipamorelin: The First Growth Hormone Peptide That Only Boosts GH Without Other Hormones.” European journal of endocrinology.Study breakdown →PubMed →↩
- 6RPEP-14810·Badran, Ahmed Samy et al. (2026). “Tesamorelin Reduces Belly Fat and Liver Fat in HIV Patients: Meta-Analysis of Trials.” Obesity research & clinical practice.Study breakdown →PubMed →↩