PT-141 vs Viagra: Two Different Erectile Mechanisms
Bremelanotide and Sexual Dysfunction
5.3x longer erections
When PT-141 was combined with sildenafil, men had erections lasting 5.3 times longer than with sildenafil alone, demonstrating synergy between central and peripheral pathways.
Diamond et al., 2005
Diamond et al., 2005
If you only read one thing
Viagra and PT-141 both produce erections, but they target opposite ends of the body. Viagra works at the penis — it makes blood flow better, but only if your brain is already sending the arousal signal. PT-141 works in the brain — it starts the arousal signal itself, which is why it can also increase desire. This matters because the two drugs fail in different situations. Viagra works for about 2 in 3 men with ED. Of the 1 in 3 it doesn't help, PT-141 rescued roughly 1 in 3 of them in one trial. Combined, the two drugs produce erections 5.3 times longer than Viagra alone. Viagra is still the standard (it's a pill and has decades of safety data). PT-141 is an injection, not FDA-approved for men, and is worth considering mainly when Viagra has failed.
PT-141 (bremelanotide) and PDE5 inhibitors like sildenafil (Viagra) both produce erections, but through mechanisms that have almost nothing in common. One works from the brain down. The other works at the penis. This is not a refinement of the same approach. It is a fundamentally different biological strategy for achieving the same physiological outcome. Understanding this distinction matters because it determines which patients benefit from which drug, whether the drugs can be combined, and why PT-141 can work in men for whom Viagra has failed. For the full clinical evidence on PT-141 in men, see PT-141 for Male Erectile Dysfunction: Research Beyond Its Approved Use. For background on how the peptide was originally discovered, see Vyleesi for Women: The Clinical Evidence on Hypoactive Sexual Desire.
Key Takeaways
- Viagra and PT-141 both produce erections, but they work at opposite ends of the body — one at the penis, the other in the brain.
- Viagra doesn't actually start an erection. It just prevents your body from ending one too soon, which only helps if your brain is already sending the arousal signal.
- PT-141 creates the arousal signal itself. That's why it's the only one of the two that also increases desire, not just physical response.
- Of the men where Viagra failed, about 1 in 3 responded to PT-141 — a rescue pathway that makes sense because it fixes a different problem.
- Combined, the two drugs produced erections over 5 times longer than Viagra alone. The mechanisms stack rather than compete.
- Viagra is a pill with decades of safety data and works for roughly 2 in 3 men with ED. It stays the first-line option for good reason.
- PT-141 is an injection, not FDA-approved for men in the US. It's really for when the standard path hasn't worked, not instead of it.
The Peripheral Pathway: How PDE5 Inhibitors Work
Sexual stimulation triggers the release of nitric oxide (NO) from nerve endings and endothelial cells in the corpus cavernosum of the penis. NO activates the enzyme guanylate cyclase, which produces cyclic GMP (cGMP). cGMP relaxes smooth muscle cells in the penile arteries and sinusoidal spaces, increasing blood flow and producing an erection.
The erection is terminated when phosphodiesterase type 5 (PDE5) breaks down cGMP. PDE5 inhibitors block this enzyme, allowing cGMP to accumulate and prolonging the erection.
Key features of this mechanism:
- It requires sexual stimulation to initiate. PDE5 inhibitors do not start the process; they amplify and sustain it.
- It acts locally in the penis. The drug has minimal direct effect on the brain.
- It does not affect sexual desire. A man on sildenafil who is not aroused will not get an erection.
- It works best when the vascular supply to the penis is intact. In conditions where blood flow is severely compromised (advanced diabetes, severe atherosclerosis), PDE5 inhibitors become less effective.
PDE5 inhibitors work in approximately 60-70% of men with ED. The 30-40% who do not respond typically have severe vascular disease, neurogenic ED, or psychological/desire-based causes that a blood flow enhancer cannot address.
The Central Pathway: How PT-141 Works
PT-141 activates melanocortin receptors (MC3R and MC4R) in the hypothalamus, specifically in the paraventricular nucleus (PVN) and the medial preoptic area (MPOA). These brain regions are the command centers for sexual function. Wessells (2005) mapped the melanocortinergic control of penile erection, showing that MC4R activation in the PVN triggers descending oxytocin and dopaminergic signals through the spinal cord to the sacral parasympathetic outflow, ultimately producing erection.[3]
Key features of this mechanism:
- It initiates the arousal process from the top. PT-141 does not just amplify an existing signal; it creates the signal.
- It affects both desire and physical response. Men in clinical trials reported increased subjective sexual desire alongside improved erections.[1]
- It does not depend on local penile vascular function. Because the drug acts upstream of the vascular response, it can work even when penile blood flow is compromised.
- It produces erection through the same neural pathways that produce naturally occurring erections (psychogenic erections), rather than artificially enhancing the downstream mechanics.
Pfaus and colleagues (2022) published a comprehensive review of bremelanotide's neurobiology, detailing how MC4R activation coordinates a complex response involving oxytocin release, dopaminergic signaling, and descending autonomic pathways to produce both the subjective experience of desire and the physiological erectile response.[8]
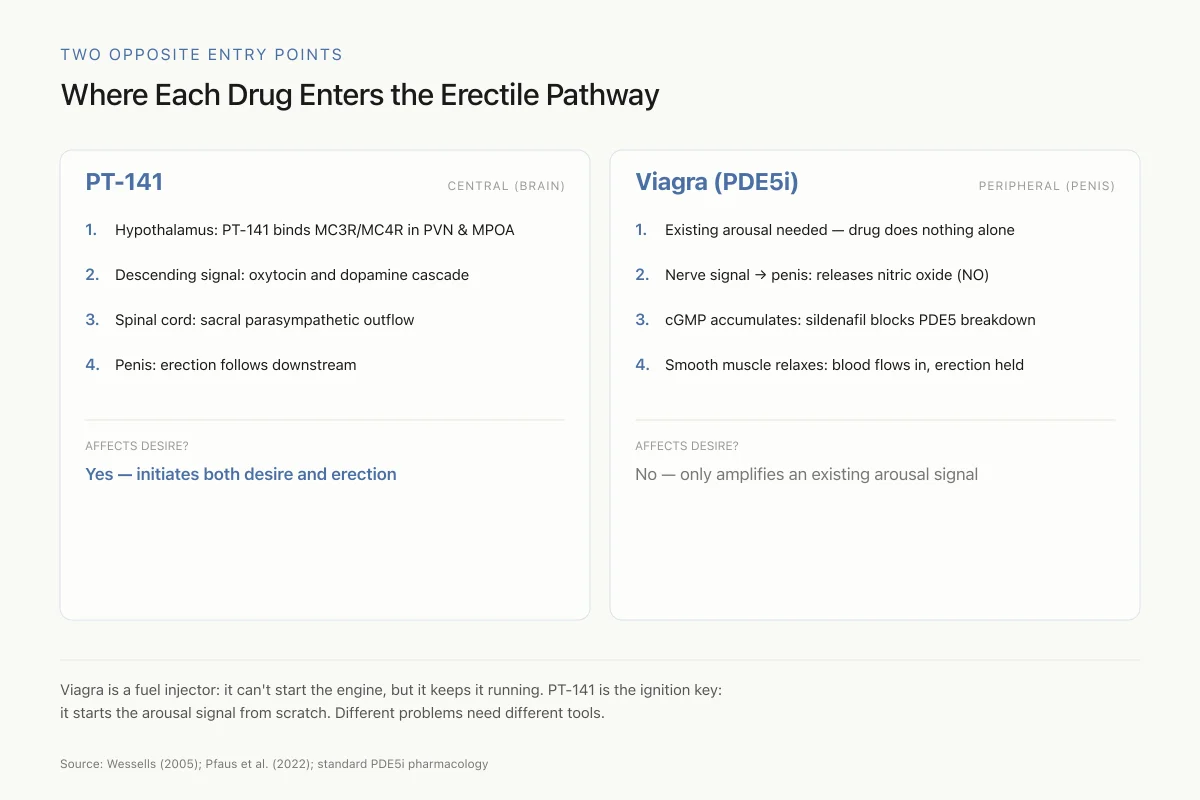
Two Opposite Entry Points
Where Each Drug Enters the Erectile Pathway
- 1.Hypothalamus: PT-141 binds MC3R/MC4R in PVN and MPOA
- 2.Descending signal: oxytocin and dopamine cascade
- 3.Spinal cord: sacral parasympathetic outflow
- 4.Penis: erection follows downstream
- 1.Existing arousal needed — drug does nothing alone
- 2.Nerve signal → penis: releases nitric oxide (NO)
- 3.cGMP accumulates: sildenafil blocks PDE5 from breaking it down
- 4.Smooth muscle relaxes: blood flows in, erection sustained
Viagra is a fuel injector: it can't start the engine, but it keeps it running. PT-141 is the ignition key: it starts the arousal signal from scratch. When the problem is "no signal," Viagra can't fix it. When the problem is "signal is fine but blood flow is weak," PT-141 alone can't fix it either.
Source: Wessells (2005); Pfaus et al. (2022); standard PDE5i pharmacology
 View as image
View as imageA Head-to-Head Comparison
| Feature | PT-141 (Bremelanotide) | PDE5 Inhibitors (Sildenafil/Tadalafil) |
|---|---|---|
| Mechanism | Central (brain MC3R/MC4R) | Peripheral (penile PDE5) |
| Site of action | Hypothalamus (PVN, MPOA) | Corpus cavernosum smooth muscle |
| Affects desire? | Yes | No |
| Requires stimulation? | Can initiate arousal | Requires existing stimulation |
| Route | Subcutaneous injection | Oral pill |
| Onset | ~30 minutes | 30-60 minutes |
| Duration | Several hours | 4-36 hours (varies by drug) |
| FDA-approved for male ED? | No | Yes (all four PDE5 inhibitors) |
| Works in PDE5 non-responders? | 34% response rate | N/A |
| Key side effects | Nausea, BP elevation, flushing | Headache, flushing, visual changes |
| Drug interactions | Limited data | Contraindicated with nitrates |
When One Drug Fails, the Other May Work
The most clinically significant implication of the mechanistic difference is that PT-141 and PDE5 inhibitors have non-overlapping failure modes.
PDE5 inhibitor failure typically occurs because the problem is upstream of the vascular pathway. Neurogenic ED (from diabetes-related nerve damage, spinal cord injury, or post-prostatectomy nerve damage), psychogenic ED (from depression, anxiety, or relationship factors), and desire-based dysfunction (low libido) all involve deficits in the neural drive that initiates erection, not in the vascular mechanics that produce it. A drug that enhances blood flow cannot fix a problem with the signal that tells blood flow to increase.
Safarinejad (2008) tested this directly. In 342 men who had failed sildenafil, intranasal PT-141 (10 mg) produced a 34% response rate versus 9% on placebo. These were men for whom the peripheral pathway approach had been proven inadequate. The fact that a central pathway agonist rescued more than a third of them suggests their ED was at least partly neural or desire-based rather than purely vascular.[5]
PT-141 failure would theoretically occur when the problem is purely downstream. If a man has severe penile vascular disease (the arteries simply cannot deliver enough blood, regardless of neural signaling), then activating the brain's arousal pathways may not be sufficient. In this case, a PDE5 inhibitor, which directly enhances the vascular response at the target organ, is the logical choice.
Combination: Central + Peripheral
Diamond and colleagues (2005) tested co-administration of intranasal PT-141 (7.5 mg) with oral sildenafil (25 mg) in men with ED. The combination produced erectile responses lasting 5.3 times longer than sildenafil alone. Both drugs were well tolerated together, with no adverse pharmacodynamic interaction.[4]
This result is pharmacologically expected. PT-141 turns on the neural arousal pathway (the ignition). Sildenafil enhances the vascular response to that neural signal (the fuel injection). Together, they address both the upstream and downstream components of erection. Shadiack and colleagues (2007) noted that the melanocortin system represents the only pharmacologically accessible central pathway for sexual function, making it the natural complement to peripheral vascular treatments.[7]
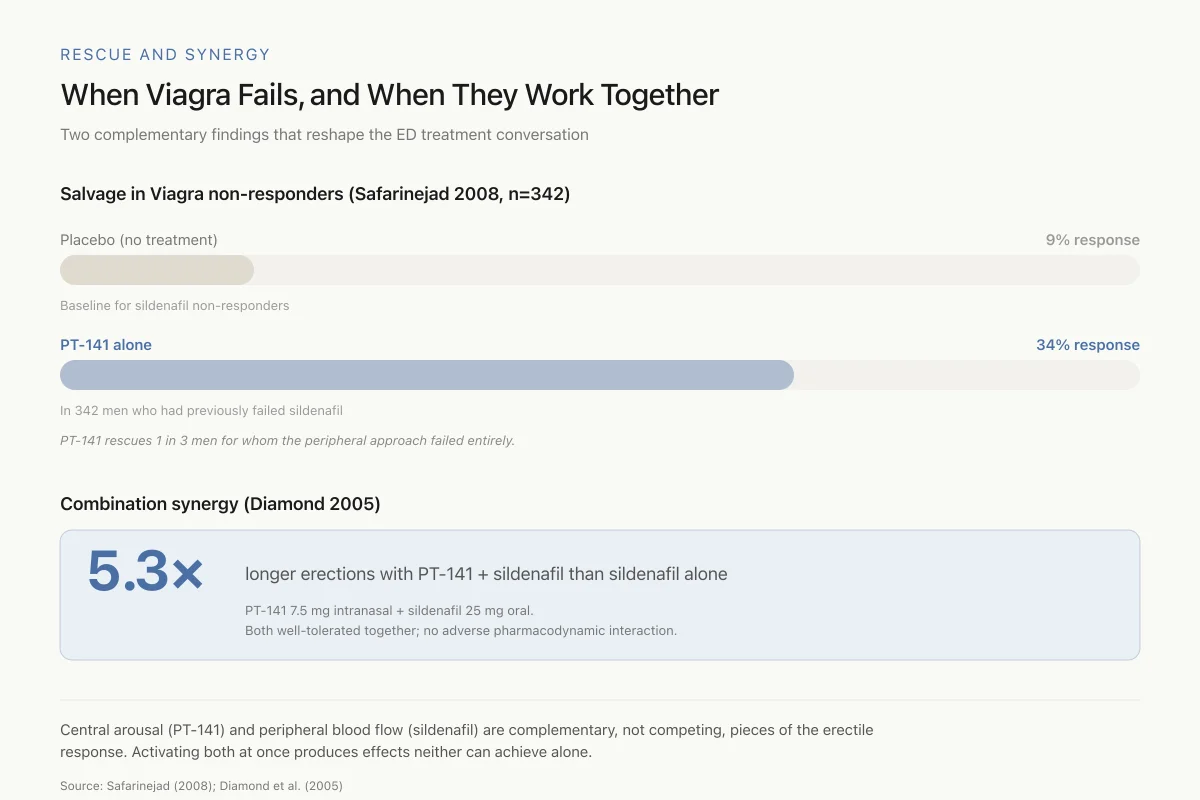
Rescue and Synergy
When Viagra Fails, and When They Work Together
Two complementary findings that reshape the ED treatment conversation
Baseline for sildenafil non-responders
In 342 men who had previously failed sildenafil
PT-141 rescues 1 in 3 men for whom the peripheral approach failed entirely.
PT-141 7.5 mg intranasal + sildenafil 25 mg oral. Both well-tolerated together; no adverse pharmacodynamic interaction.
Central arousal (PT-141) and peripheral blood flow (sildenafil) are complementary — not competing — pieces of the erectile response. Activating both at once produces effects neither can achieve alone.
Source: Safarinejad (2008); Diamond et al. (2005)
 View as image
View as imageThe combination data suggests that some men classified as "PDE5 non-responders" may actually have partial peripheral responses that become clinically meaningful only when combined with adequate central drive.
Practical Differences: Pills vs Injections
Beyond pharmacology, PT-141 and PDE5 inhibitors differ in practical terms that affect patient acceptance.
PDE5 inhibitors are oral pills. They are convenient, discreet, and familiar. Sildenafil is taken 30-60 minutes before sexual activity. Tadalafil can be taken daily at low doses (5 mg) for continuous coverage, eliminating the need to plan around dosing.
PT-141 (as currently formulated in Vyleesi) is a subcutaneous injection in the abdomen or thigh, administered at least 45 minutes before sexual activity. For many men, self-injection before sex is a significant practical and psychological barrier, especially when an oral alternative exists. This delivery limitation is one reason the drug was not pursued for male ED approval.
Ila and colleagues (2025) reviewed intravenous peptides and amino acids for erectile dysfunction, noting that injection-based approaches face adoption challenges but may offer efficacy in populations unresponsive to oral therapies.[9]
Safety Profiles
PDE5 inhibitors have decades of post-marketing safety data. The main risks are headache, flushing, nasal congestion, visual disturbances (sildenafil), and back pain (tadalafil). The critical safety concern is the absolute contraindication with nitrate medications: combining PDE5 inhibitors with nitrates can cause dangerous hypotension. Men on nitroglycerin for angina cannot use PDE5 inhibitors.
PT-141 causes nausea (the most common side effect), facial flushing, and transient blood pressure elevation. The blood pressure effect is the opposite of PDE5 inhibitors (which tend to lower blood pressure slightly). In the male ED population, which has high rates of hypertension and cardiovascular disease, transient blood pressure elevation is a more significant concern than in the premenopausal female HSDD population for which the drug was approved. Uckert and colleagues (2014) summarized the safety profile across male and female studies, noting that nausea was dose-related and generally self-limited.[6]
Importantly, PT-141 is not contraindicated with nitrates. Because it does not affect the nitric oxide/cGMP pathway, it can theoretically be used in men who cannot take PDE5 inhibitors due to nitrate use. This represents a genuinely unmet clinical need, though no clinical trial has specifically tested PT-141 in this population. For a complete overview of PT-141's side effect profile, see PT-141 Side Effects: Nausea, Blood Pressure, and Skin Darkening.
Safety
ModerateOpposite blood pressure effects — matters more for male ED population
Concern
PT-141 transiently raises blood pressure. PDE5 inhibitors slightly lower it. Male ED patients skew older and have high rates of hypertension and cardiovascular disease. A drug that raises BP in a population already managing BP is a different risk-benefit calculation than it is for the premenopausal women PT-141 was approved for.
What the research says
PT-141's BP effect is transient (hours) and dose-related. It is not contraindicated with antihypertensives. But clinicians and patients need to know it's not pharmacologically 'safer' than Viagra in a cardiovascular sense — it just has different risks.
Particularly relevant for: Men with hypertension, cardiovascular disease, or on multiple BP-affecting medications
What to do
If you have CVD risk factors, baseline and on-dose BP monitoring is appropriate. Don't assume PT-141 is the 'heart-safe' alternative to Viagra just because it skips the nitric oxide pathway.
Uckert et al. (2014); Vyleesi prescribing information
Evidence Summary
The Bottom Line
PT-141 and PDE5 inhibitors target opposite ends of the erectile pathway. PDE5 inhibitors enhance penile blood flow by blocking cGMP breakdown. PT-141 activates melanocortin receptors in the hypothalamus, initiating the neural cascade that produces both desire and erection. This mechanistic difference means PT-141 can work in men who fail PDE5 inhibitors (34% response rate in one trial), and combining both approaches produces synergistic effects (5.3x longer erections). PDE5 inhibitors remain the standard of care because they are oral, well-studied, and effective in the majority of men. PT-141 is not approved for male ED and requires subcutaneous injection, limiting its practical adoption.
Sources & References
- 1RPEP-00849·Molinoff, P B et al. (2003). “PT-141: A Melanocortin Peptide That Treats Sexual Dysfunction Through the Brain.” Annals of the New York Academy of Sciences.Study breakdown →PubMed →↩
- 2RPEP-00903·Diamond, L E et al. (2004). “PT-141 Nasal Spray Safely Induces Erection in Both Healthy Men and ED Patients.” International journal of impotence research.Study breakdown →PubMed →↩
- 3RPEP-01100·Wessells, H et al. (2005). “Melanocortinergic control of penile erection..” Peptides.Study breakdown →PubMed →↩
- 4RPEP-01028·Diamond, L E et al. (2005). “Combining Low-Dose PT-141 Nasal Spray With Viagra: Synergistic Erectile Effect.” Urology.Study breakdown →PubMed →↩
- 5RPEP-01413·Safarinejad, Mohammad Reza et al. (2008). “Bremelanotide Rescues Men Who Fail Viagra: A Brain Approach When Blood Flow Drugs Don't Work.” The Journal of urology.Study breakdown →PubMed →↩
- 6RPEP-02565·Ückert, Stefan et al. (2014). “Melanocortin Peptide Agonists Show Promise for Treating Sexual Dysfunction in Both Men and Women Through Central Brain Pathways.” Expert opinion on investigational drugs.Study breakdown →PubMed →↩
- 7RPEP-01288·Shadiack, Annette M et al. (2007). “Melanocortins for Both Male AND Female Sexual Dysfunction: PT-141 and Beyond.” Current topics in medicinal chemistry.Study breakdown →PubMed →↩
- 8RPEP-06431·Pfaus, James G et al. (2022). “The neurobiology of bremelanotide for the treatment of hypoactive sexual desire disorder in premenopausal women..” CNS spectrums.Study breakdown →PubMed →↩
- 9RPEP-11513·Ila, Vishal et al. (2025). “Intravenous peptides and amino acids for erectile dysfunction: a narrative review of current applications and future directions..” Expert opinion on pharmacotherapy.Study breakdown →PubMed →↩