Collagen Peptides for Athletes: Tendon and Ligament Data
Collagen for Exercise-Induced Joint Pain
15 g/day
The dose most commonly used in clinical trials showing tendon remodeling and joint improvement in athletes, typically taken 30-60 minutes before exercise with vitamin C.
Konig et al., Applied Physiology, Nutrition, and Metabolism, 2018
Konig et al., Applied Physiology, Nutrition, and Metabolism, 2018
If you only read one thing
Collagen peptides are one of the few connective-tissue supplements with real human trial data behind them. At 15 grams a day, with 50 mg of vitamin C, taken 30 to 60 minutes before training, they've been shown to thicken tendons, raise tendon stiffness, and reduce knee pain in active adults over 12 to 24 weeks. They don't build muscle the way whey does — they help the rope (tendons, ligaments, joints), not the engine (muscle fiber). And no study has proven they prevent injuries. They help the tissue that holds you together, not the one that moves you.
Collagen is the most abundant protein in the human body, comprising approximately 30% of total protein content. Tendons and ligaments are 65-80% collagen by dry weight, predominantly type I collagen organized into hierarchical fiber bundles that withstand enormous tensile forces. When athletes supplement with collagen peptides (hydrolyzed collagen broken into fragments of 2-10 kilodaltons), the hypothesis is straightforward: provide the building blocks to support connective tissue repair and adaptation. For the broader evidence on collagen and exercise-related joint pain, see our pillar guide to collagen for exercise-induced joint pain.
The clinical evidence has matured considerably since the early observational reports. A 2024 meta-analysis of 19 studies with 768 participants found statistically significant effects of collagen peptide supplementation on tendon morphology, fat-free mass, and 48-hour recovery in reactive strength following exercise-induced muscle damage. But the certainty of evidence was rated very low for tendon and mechanical outcomes, and the practical significance of the observed changes for injury prevention remains unconfirmed. Replication has been inconsistent: some studies show clear benefits while others find no significant difference versus placebo, creating a literature that resists simple summary. This article examines the specific evidence for tendon and ligament effects in athletic populations.
Key Takeaways
- Your tendons and ligaments are built mostly of collagen — about 70% of their dry weight — which is why athletes started paying attention.
- In trials, 15 grams a day for 12 to 24 weeks made tendons thicker and stiffer, and reduced knee pain in active adults.
- When you eat collagen, small fragments actually reach your tendons within 1 to 2 hours — which is why the pre-workout timing matters.
- Collagen is not a muscle-builder. It's low in leucine, the amino acid that triggers muscle growth. Think ropes, not engine.
- Stiffer tendons have translated into measurably better explosive strength — things like jumping and sprinting — in at least one 16-week trial.
- No study has actually proven collagen prevents injuries. That trial would need thousands of athletes tracked for years.
- Take it 30 to 60 minutes before training with 50 mg of vitamin C — the vitamin C is what lets your body actually build collagen.
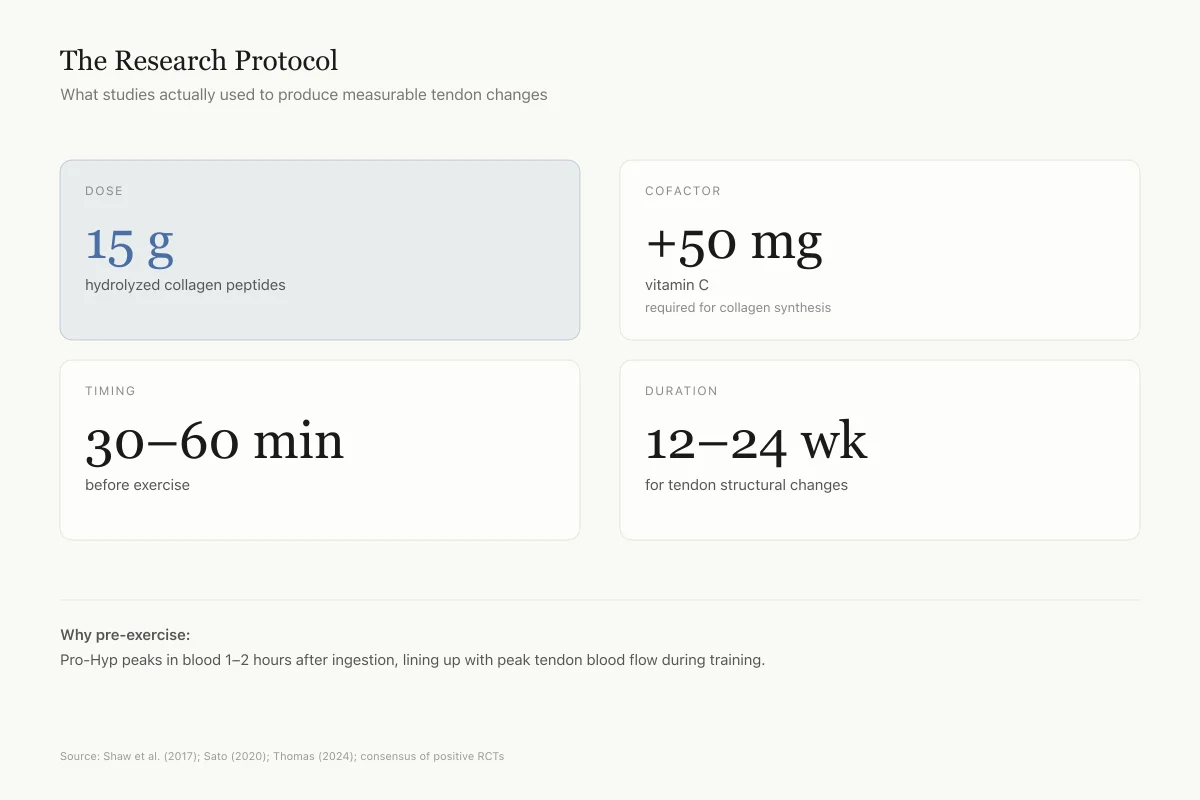
The Research Protocol
What Studies Actually Used
The dose, timing, and duration that produced measurable tendon changes
Dose
15 g
hydrolyzed collagen peptides
Cofactor
+50 mg
vitamin C (required for collagen synthesis)
Timing
30–60 min
before exercise
Duration
12–24 weeks
for tendon structural changes
Why pre-exercise: the collagen metabolite Pro-Hyp peaks in blood 1–2 hours after ingestion, lining up with peak tendon blood flow during training. The tissue gets more of the circulating fragments when the timing is right.
Source: Shaw et al. (2017); Sato (2020); Thomas (2024); consensus of positive RCTs
 View as image
View as imageHow Oral Collagen Reaches Tendons
The first question in collagen supplementation is whether ingested peptides actually reach their target tissues. Collagen peptides are hydrolyzed during digestion into dipeptides and tripeptides, primarily prolyl-hydroxyproline (Pro-Hyp) and hydroxyprolyl-glycine (Hyp-Gly). These fragments are absorbed intact through intestinal peptide transporters (particularly PepT1) and enter the bloodstream.
A 2020 study demonstrated that Pro-Hyp accumulates in connective tissues after oral administration, and that this dipeptide stimulates fibroblast proliferation and collagen synthesis in vitro. The concentration of Pro-Hyp in blood peaks 1-2 hours after ingestion, which is the rationale for the common recommendation to take collagen 30-60 minutes before exercise: the exercise-induced increase in tendon blood flow may enhance local delivery of circulating peptides to the stressed tissue.[8]
A 2016 study confirmed that bioactive collagen hydrolysate fragments can be detected in human blood after oral ingestion, with specific peptide fragments reaching concentrations sufficient to stimulate collagen-producing cells in culture.[9]
The biological plausibility is established: collagen peptides are absorbed, circulate as bioactive fragments, and can stimulate collagen-producing cells. Whether this translates to meaningful structural changes in human tendons and ligaments at supplemental doses is the question addressed by clinical trials.
The Tendon Remodeling Evidence
The most compelling evidence for collagen's effects on tendons comes from studies combining supplementation with exercise.
A 2024 meta-analysis synthesized data from multiple trials examining collagen peptide supplementation during resistance training programs. Tendon cross-sectional area (primarily patellar tendons) was significantly increased in the collagen groups compared to placebo, indicating structural remodeling. The effect was most pronounced after 12 or more weeks of combined supplementation and training.[5]
A 2025 randomized controlled trial provided the strongest evidence to date. Miyamoto and colleagues randomized healthy young males to 16 weeks of collagen peptide supplementation or placebo alongside a resistance training program. The collagen group showed increased muscle-tendon unit stiffness and improved explosive strength compared to placebo. The enhancement of tendon stiffness appeared to directly contribute to improved rate of force development, a critical performance metric for sprinting, jumping, and change-of-direction sports.[7]
A 2024 study specifically examined collagen supplementation before exercise and found that pre-exercise timing enhanced markers of collagen synthesis compared to supplementation at other times, supporting the timing-dependent delivery hypothesis.[6]
These structural findings are promising but need context. The meta-analysis rated the certainty of evidence for tendon morphology as "very low," meaning future studies could substantially change the estimate. Tendon cross-sectional area is a surrogate measure; whether the observed thickening translates to reduced injury rates has not been established in any trial. The comparison to BPC-157 for tendon injuries, which has extensive preclinical but no human clinical data, highlights how collagen peptides occupy a unique position: more clinical evidence than most peptide interventions, but still insufficient for definitive injury prevention claims.
Timeline of Effects
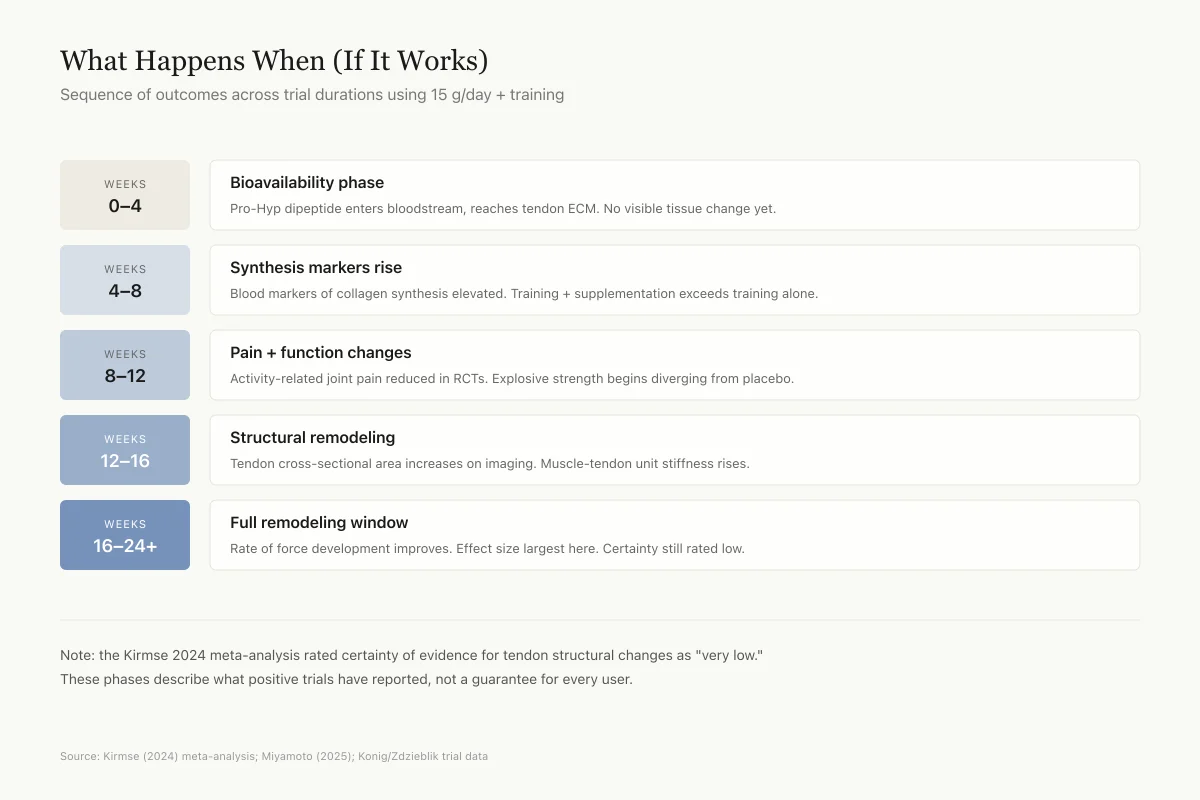
What Happens When (If It Works)
Sequence of outcomes across trial durations using 15 g/day + training
Weeks
0–4
Bioavailability phase
Pro-Hyp dipeptide enters bloodstream, reaches tendon ECM. No visible tissue change yet.
Weeks
4–8
Synthesis markers rise
Blood markers of collagen synthesis elevated. Training + supplementation stacks exceed training alone.
Weeks
8–12
Pain + function changes
Activity-related joint pain reduced in RCTs. Explosive strength begins diverging from placebo.
Weeks
12–16
Structural remodeling
Tendon cross-sectional area increases on imaging. Muscle-tendon unit stiffness rises.
Weeks
16–24+
Full remodeling window
Rate of force development improves. Effect size largest here. Certainty still rated low.
Note: the Kirmse 2024 meta-analysis rated certainty of evidence for tendon structural changes as "very low." These phases describe what positive trials have reported, not a guarantee that every user experiences them.
Source: Kirmse (2024) meta-analysis; Miyamoto (2025); Konig/Zdzieblik trial data
 View as image
View as imageJoint Pain and Functional Outcomes
The evidence for collagen peptides reducing joint pain in athletes is stronger and more consistent than the structural tendon data.
A 2018 double-blind, placebo-controlled trial randomized 139 physically active young adults (without diagnosed joint disease) to receive 5 g of specific collagen peptides or placebo daily for 12 weeks. The collagen group reported significantly reduced activity-related knee joint discomfort compared to placebo, with effects measured by visual analog scale and validated joint function questionnaires.[1]
A 2023 study of collagen peptide supplementation in active individuals confirmed improvements in joint comfort and physical function scores, with the benefits most apparent during and after high-impact activities.[4]
A 2021 systematic review of collagen's effects on joint health, body composition, and exercise recovery found moderate evidence supporting joint pain reduction in athletic populations, but noted that the mechanisms remained incompletely understood and that many trials had methodological limitations including small sample sizes and industry funding.[3]
For athletes, the practical question is whether collagen supplementation can reduce the joint pain and stiffness that accumulate over training cycles, allowing higher training volumes and better performance over time. The evidence supports a modest benefit for activity-related discomfort, particularly in the knee. Whether this reflects structural improvement (cartilage or synovial membrane repair) or an analgesic/anti-inflammatory effect of collagen fragments circulating through inflamed tissue is unclear. Both mechanisms may contribute. Collagen-derived peptides have been shown to inhibit MMP activity (the enzymes that degrade cartilage) in vitro, while simultaneously stimulating chondrocyte collagen synthesis. This dual action could slow joint degradation while promoting repair, though demonstrating this in vivo at supplemental doses remains an open challenge. The broader evidence on collagen for exercise-induced joint pain covers this question in greater depth.
Body Composition and Recovery
Beyond tendons and joints, athletes are interested in whether collagen peptides affect muscle mass and recovery. The connective tissue matrix surrounding muscle fibers (the extracellular matrix, or ECM) is itself predominantly collagen, and ECM remodeling is a recognized component of muscle adaptation to training. Disruption of the muscular ECM contributes to exercise-induced muscle damage, and its repair requires collagen synthesis.
A 2015 randomized controlled trial studied collagen peptide supplementation (15 g/day) combined with resistance training in elderly men with sarcopenia. The collagen group gained significantly more fat-free mass and lost more fat mass than the placebo group after 12 weeks of training.[2] While this population differs from young athletes, the mechanism (stimulation of muscle protein synthesis via mTOR pathway activation by collagen-derived peptides, particularly the unique amino acid hydroxyproline) could apply broadly across age groups, though the effect magnitude in already well-nourished young athletes is likely smaller.
A 2024 meta-analysis confirmed small but statistically significant effects of collagen supplementation on fat-free mass and 48-hour recovery of reactive strength following exercise-induced muscle damage. The recovery benefit is particularly relevant for athletes in sports requiring repeated high-intensity efforts across multi-day competitions or dense training schedules.
A 2026 study of low-molecular-weight collagen peptide supplementation provided additional evidence for improved connective tissue recovery markers in exercising adults, with benefits appearing to be dose-dependent.[10]
For muscle recovery specifically, collagen peptides appear to offer modest benefits that may complement (not replace) whey or essential amino acid supplementation. Collagen is low in leucine, the primary amino acid trigger for muscle protein synthesis, which limits its direct muscle-building potential compared to complete protein sources. Its value for athletes likely lies in the connective tissue compartment rather than contractile muscle. For a deeper analysis, see does collagen help muscle recovery after exercise.
Protein Source Comparison
What Each Protein Actually Helps Build
Collagen and whey target different tissues — they complement, not replace
| Tissue | Whey | Collagen |
|---|---|---|
Contractile muscle fiber Whey is leucine-rich; collagen is leucine-poor | Strong | Weak |
Muscle extracellular matrix ECM is collagen-based; supplementation aids repair | Weak | Moderate |
Tendons Pro-Hyp accumulates in tendon tissue | Weak | Moderate |
Ligaments Similar biology to tendons; less trial data | Weak | Moderate |
Cartilage / joint surfaces Some evidence of MMP inhibition + chondrocyte stimulation | Weak | Moderate |
Recovery after muscle damage Whey drives protein synthesis; collagen aids ECM repair | Strong | Moderate |
Source: Khatri (2021) review; Kirmse (2024) meta-analysis; Zdzieblik (2015); Kviatkovsky (2023)
Dosing, Timing, and the Vitamin C Question
Most positive clinical trials use 5-15 g of hydrolyzed collagen per day. The emerging consensus favors 15 g as the dose most likely to produce measurable effects on connective tissue, based on the accumulation of pharmacokinetic and outcome data.
Timing appears to matter. The recommendation to consume collagen 30-60 minutes before exercise is based on the pharmacokinetic peak of Pro-Hyp in blood (1-2 hours post-ingestion) coinciding with the exercise period, when tendon blood flow is maximized. A 2024 study supported this approach, showing enhanced collagen synthesis markers with pre-exercise supplementation.
Vitamin C is frequently co-administered (typically 50 mg) because it is a required cofactor for prolyl hydroxylase, the enzyme that hydroxylates proline residues during collagen synthesis. Without adequate vitamin C, collagen formation is impaired. Whether the additional 50 mg provides benefit beyond dietary adequacy is debated, but given vitamin C's low cost and safety, it remains part of most research protocols. The question of vitamin C and collagen synthesis has its own dedicated evidence base.
The source of collagen peptides varies across studies (bovine, porcine, marine), and whether the source meaningfully affects outcomes is unknown. Some evidence suggests that specific collagen peptides (selected for particular amino acid sequences) may be more effective than generic hydrolyzed collagen, but head-to-head comparisons are limited. Molecular weight also varies: most supplements contain peptides of 2-6 kDa, while some products use larger fragments. The optimal molecular weight for tendon and ligament effects has not been established.
A 2023 study using a specific low-molecular-weight collagen formulation reported improvements in joint function scores that exceeded results from earlier trials using less defined hydrolysates, suggesting that peptide specificity may matter.[4] This raises questions about whether the generic "collagen peptide" label used by most supplements is precise enough. Collagen hydrolysates from different sources and different enzymatic processes produce different peptide profiles, which may have different bioactivities.
Collagen peptides for connective tissue represent a different therapeutic approach than other peptide interventions being studied for joint and tendon health. While BPC-157 has preclinical tendon data but no human trials, collagen peptides have multiple human RCTs but less dramatic preclinical mechanistic evidence. The overlap with collagen peptides for bone density and elastin peptides in skin suggests that dietary peptide supplementation may influence the extracellular matrix across multiple tissue types, not just tendons and ligaments.
The Bottom Line
Collagen peptide supplementation for athletes has graduated from theoretical to evidence-supported, though the evidence remains early-stage for some endpoints. Joint pain reduction in active individuals is the best-established benefit, supported by multiple placebo-controlled trials. Tendon structural remodeling (increased cross-sectional area and stiffness) has been observed in meta-analyses and a 2025 RCT, with corresponding improvements in explosive strength. The practical translation to injury prevention has not been demonstrated. For athletes seeking an evidence-based connective tissue support strategy, 15 g of collagen peptides with vitamin C taken before exercise represents the protocol best supported by current data.
Sources & References
- 1RPEP-03765·König, Daniel et al. (2018). “Collagen Peptide Supplements Increased Bone Density in Postmenopausal Women Over 12 Months.” Nutrients.Study breakdown →PubMed →↩
- 2RPEP-02845·Zdzieblik, Denise et al. (2015). “Collagen peptide supplementation in combination with resistance training improves body composition and increases muscle strength in elderly sarcopenic men: a randomised controlled trial..” The British journal of nutrition.Study breakdown →PubMed →↩
- 3RPEP-05493·Khatri, Mishti et al. (2021). “The effects of collagen peptide supplementation on body composition, collagen synthesis, and recovery from joint injury and exercise: a systematic review..” Amino acids.Study breakdown →PubMed →↩
- 4RPEP-07070·Kviatkovsky, Shiloah A et al. (2023). “9-Month Trial: Collagen Peptide Supplements Improve Pain, Function, and Mental Health in Active Middle-Aged Adults.” Journal of the International Society of Sports Nutrition.Study breakdown →PubMed →↩
- 5RPEP-08561·Kirmse, Marius et al. (2024). “Collagen Peptide Supplementation during Training Does Not Further Increase Connective Tissue Protein Synthesis Rates..” Medicine and science in sports and exercise.Study breakdown →PubMed →↩
- 6RPEP-09380·Thomas, Craig et al. (2024). “Collagen Peptides Before Bed Reduce Sleep Disruptions and Improve Next-Day Cognitive Function.” European journal of nutrition.Study breakdown →PubMed →↩
- 7RPEP-12594·Miyamoto, Naokazu et al. (2025). “Collagen Peptide Supplementation Enhances Muscle-Tendon Stiffness and Explosive Strength: A 16-wk Randomized Controlled Trial..” Medicine and science in sports and exercise.Study breakdown →PubMed →↩
- 8RPEP-05111·Sato, Kenji et al. (2020). “Collagen Dipeptide Pro-Hyp Identified as Growth Signal for Wound-Healing Fibroblasts.” Frontiers in cell and developmental biology.Study breakdown →PubMed →↩
- 9RPEP-02975·Inoue, Naoki et al. (2016). “Collagen Peptide Supplements Improve Skin Moisture, Elasticity, and Wrinkles in Randomized Controlled Trial.” Journal of the science of food and agriculture.Study breakdown →PubMed →↩
- 10RPEP-15340·Hwang, Sehee et al. (2026). “Fish Collagen Peptides Reduce Cellulite and Thicken Hair in 24-Week RCT of 114 Women.” Journal of medicinal food.Study breakdown →PubMed →↩