GHK-Cu for Skin: What the Evidence Shows
GHK-Cu Copper Peptide
70% collagen improvement
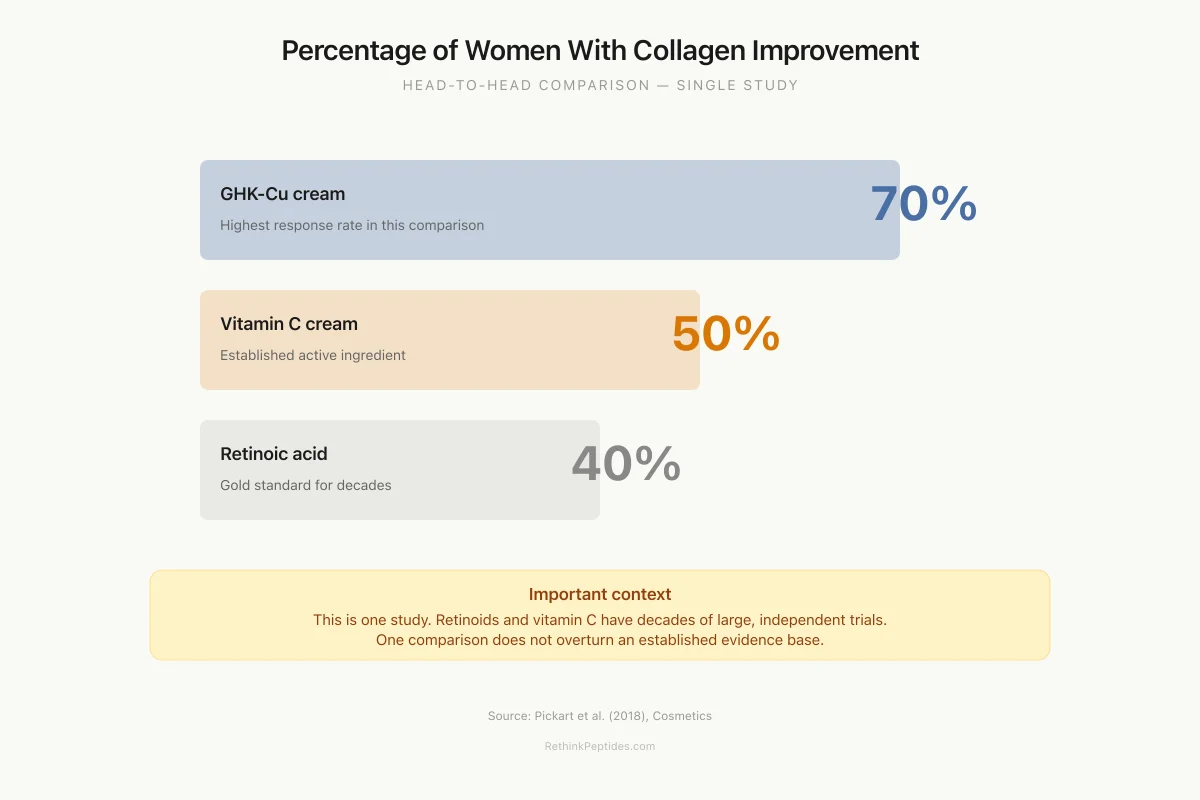
In a comparative clinical study, topical GHK-Cu improved collagen production in 70% of women treated, versus 50% for vitamin C cream and 40% for retinoic acid.
Pickart et al., Cosmetics, 2018
Pickart et al., Cosmetics, 2018
If you only read one thing
GHK-Cu is a tiny copper-binding peptide your body naturally makes. At age 20, you have plenty of it — by 60, you've lost 60%. In lab studies, it's shockingly potent at boosting collagen, even at concentrations a billion times smaller than most drugs. Clinical studies show real wrinkle reduction and better collagen than vitamin C or retinoids. The catch: those studies are small, mostly industry-funded, and we still don't know for sure how much actually gets through your skin when you rub it on.
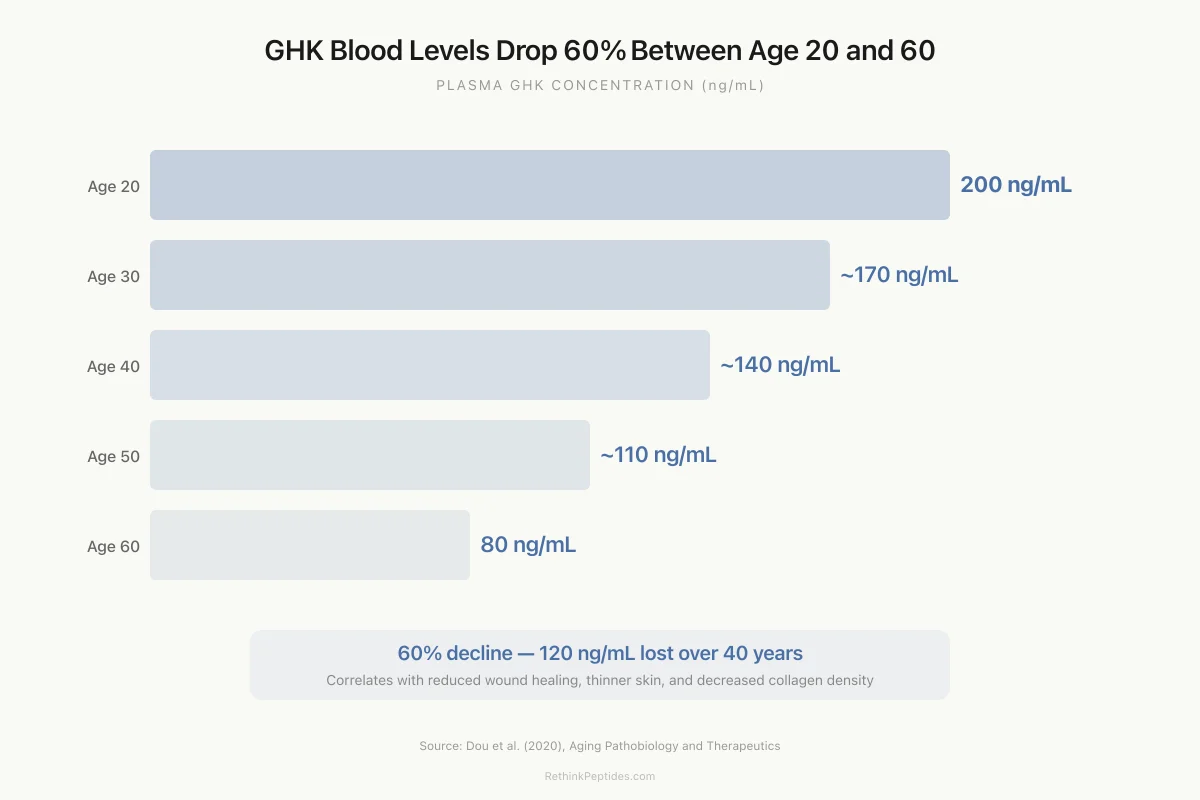
GHK-Cu (glycyl-L-histidyl-L-lysine copper complex) is a tripeptide naturally present in human blood plasma at concentrations averaging 200 ng/mL at age 20, declining to approximately 80 ng/mL by age 60.[2] It is one of the few peptides that has crossed the boundary from laboratory research into widespread commercial skincare products, appearing in serums, creams, and post-procedure treatments marketed for anti-aging effects. The commercial enthusiasm is grounded in real science: GHK-Cu stimulates collagen synthesis at extraordinarily low concentrations (picomolar), modulates thousands of human genes, and has shown measurable wrinkle reduction in clinical studies. But the clinical evidence base is thinner than the marketing suggests, and critical questions about skin penetration, optimal formulation, and long-term outcomes remain unanswered. This article evaluates what the research actually shows. For more focused coverage, see the cluster articles on GHK-Cu for wrinkles and collagen synthesis, topical copper peptide rejuvenation, GHK-Cu and skin barrier repair, and GHK-Cu and photodamage protection.
Key Takeaways
- GHK-Cu was discovered when young people's blood made old liver tissue behave young again.
- It triggers collagen production at concentrations so tiny they'd equal one drop in an Olympic swimming pool.
- In a head-to-head trial, 70% improved on copper peptides versus 40% on retinoids and 50% on vitamin C.
- Compared to plain serum, copper peptides cut wrinkle volume by over half in 12 weeks.
- Almost all the strongest evidence comes from one researcher who founded a copper peptide skincare company.
- Retinoids still have decades of independent trials behind them. GHK-Cu does not.
- GHK-Cu appears to flip the switches damaged tissue uses to rebuild itself — including 47 DNA repair genes.
Discovery and basic biology
GHK was first isolated from human plasma by Loren Pickart in the 1970s. The peptide consists of just three amino acids, glycine, histidine, and lysine, with an exceptionally high affinity for copper(II) ions. In physiological conditions, it exists primarily as the copper chelate GHK-Cu. The discovery of its biological activity came from an unexpected observation: serum from young donors (age 20-25) could stimulate aged liver tissue to synthesize proteins at a rate characteristic of younger tissue, while serum from older donors (age 60-80) could not. The active factor was isolated and identified as GHK.[4]
Maquart et al. (1988) provided the foundational biochemical data. Working with fibroblast cultures, they demonstrated that GHK-Cu stimulated collagen synthesis at concentrations beginning between 10 picomolar and 100 picomolar, with peak stimulation at 1 nanomolar. The collagen increase was independent of cell number changes; GHK-Cu was making existing fibroblasts produce more collagen, not simply growing more cells.[1]
Picomolar activity is unusual for a small peptide and suggests high-affinity receptor-mediated signaling, though the specific receptor for GHK-Cu has never been identified. The GHK sequence also appears within the alpha-2(I) chain of type I collagen, leading to the hypothesis that collagen degradation at wound sites releases GHK fragments that then bind copper and signal for new collagen production, creating a self-repair feedback loop.[1]
What GHK-Cu does in cells and tissues
Pickart and colleagues have spent decades cataloguing GHK-Cu's biological effects. The 2015 review in BioMed Research International summarized the evidence across multiple tissue types.[3]
Extracellular matrix remodeling. GHK-Cu stimulates synthesis of collagen (types I and III), dermatan sulfate, chondroitin sulfate, and the small proteoglycan decorin. It also modulates metalloproteinase (MMP) activity and their inhibitors (TIMPs), influencing not just the production of new matrix but the breakdown and remodeling of existing tissue. This dual role, stimulating both synthesis and controlled degradation, is characteristic of wound healing rather than simple collagen accumulation.[3]
Cell recruitment. GHK-Cu attracts immune cells (macrophages, mast cells) and endothelial cells to injury sites, stimulates angiogenesis (new blood vessel formation), and promotes nerve outgrowth. This makes it a wound-healing signal rather than simply a cosmetic ingredient.[3]
Gene expression. Using the Broad Institute's Connectivity Map (CMap), which compares gene expression signatures across thousands of compounds, Pickart et al. (2018) found that GHK modulated the expression of over 4,000 human genes. Of particular interest: 47 DNA repair genes were stimulated and 5 were suppressed. Genes involved in antioxidant defense and the ubiquitin proteasome system were also upregulated. The overall gene expression pattern shifted cells from a profile associated with diseased or damaged tissue toward a healthier state.[5]
Anti-inflammatory and antioxidant effects. GHK-Cu has been shown to reduce markers of inflammation and oxidative stress in both cell culture and animal models. Dou et al. (2020) noted that GHK-Cu possesses prominent antioxidant and anti-inflammatory effects, and that preliminary observations suggest it can partially reverse cognitive impairment in aging mice by targeting anti-inflammatory and epigenetic pathways.[2]
Beyond skin: pulmonary fibrosis. Ma et al. (2020) demonstrated protective effects of GHK-Cu in a bleomycin-induced pulmonary fibrosis model, showing anti-oxidative stress and anti-inflammatory activity in lung tissue. This study extends GHK-Cu's relevance beyond cosmetic applications to organ-level disease models.[6]
Clinical evidence for skin
The clinical data for GHK-Cu on human skin are real but limited in scope. They come primarily from industry-sponsored cosmetic studies rather than large, independent, placebo-controlled dermatological trials.
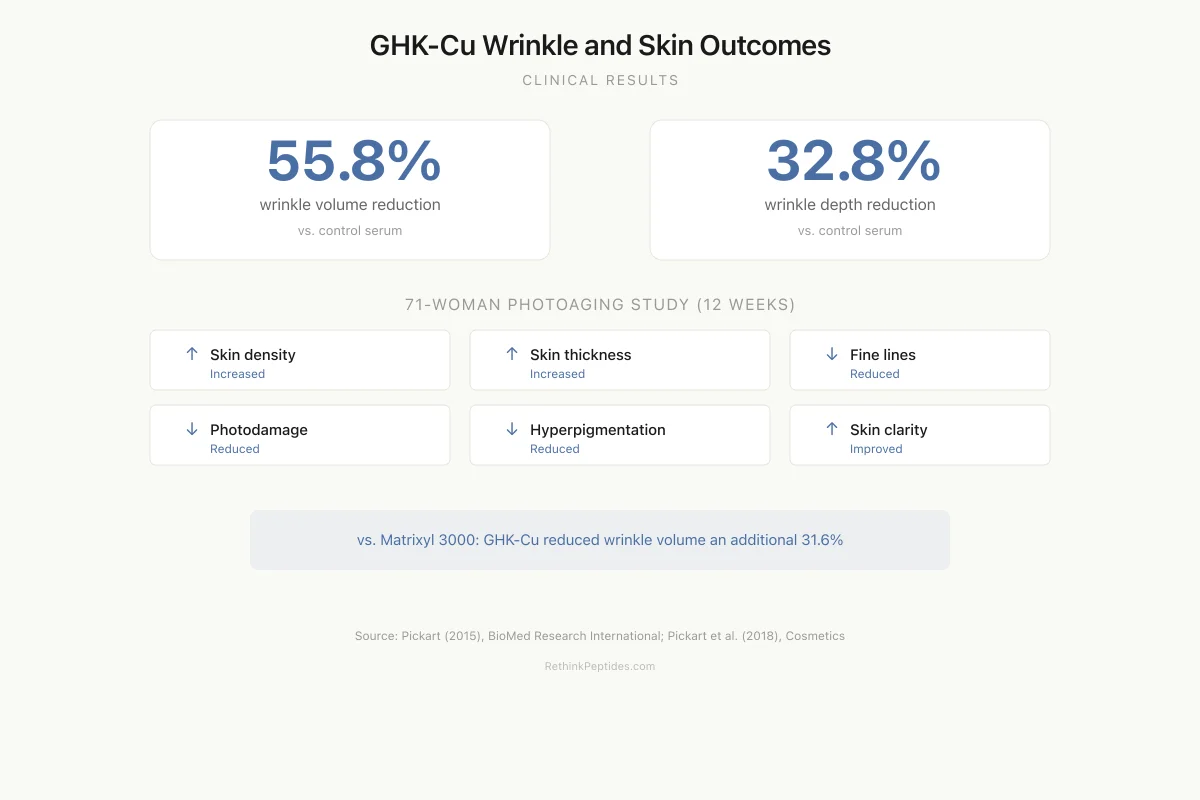
The 71-woman photoaging study. Pickart et al. (2018) reported a study in which 71 women with mild to advanced photoaging applied a facial cream containing GHK-Cu for 12 weeks. The treatment increased skin density and thickness, reduced fine lines and the depth of wrinkles, reduced photodamage and hyperpigmentation, improved skin clarity, and increased keratinocyte proliferation.[5]
The collagen comparative study. In a separate trial, topical GHK-Cu was compared head-to-head with vitamin C cream and retinoic acid for collagen improvement. GHK-Cu improved collagen production in 70% of women treated, compared to 50% for vitamin C and 40% for retinoic acid.[5] This outperformance of two established dermatological actives is notable, though the study methodology, blinding procedures, and outcome measurement techniques are not described in the level of detail that independent peer review would demand.
Head-to-Head Results
Percentage of Women With Collagen Improvement
One comparative study — not yet independently replicated
Important context: This is a single study. Retinoids and vitamin C have decades of independent evidence from large trials. GHK-Cu does not. One comparison does not overturn an established evidence base.
Source: Pickart et al. (2018), Cosmetics
 View as image
View as imageWrinkle volume measurements. When GHK-Cu was compared to Matrixyl 3000 (palmitoyl pentapeptide-4), GHK-Cu reduced wrinkle volume by 31.6%. Compared to a control serum, it reduced wrinkle volume by 55.8% and wrinkle depth by 32.8%.[3]
Clinical Results
GHK-Cu Wrinkle and Skin Outcomes
Measured wrinkle reductions
55.8%
wrinkle volume reduction
vs. control serum
32.8%
wrinkle depth reduction
vs. control serum
71-woman photoaging study (12 weeks)
Skin density
Increased
Skin thickness
Increased
Fine lines
Reduced
Photodamage
Reduced
Hyperpigmentation
Reduced
Skin clarity
Improved
Source: Pickart (2015), BioMed Res Int; Pickart et al. (2018), Cosmetics
 View as image
View as imagePost-laser resurfacing. Studies have examined GHK-Cu application after CO2 laser resurfacing and found accelerated healing and improved cosmetic outcomes, though these studies predate current clinical trial standards.
The skin penetration problem
A critical issue for topical GHK-Cu is whether the peptide actually reaches its target cells. GHK is hydrophilic (water-loving), small, and carries a charge at physiological pH. The stratum corneum, the outer layer of skin, is a lipophilic barrier designed to keep hydrophilic molecules out.
Mortazavi et al. (2025) addressed this question directly in a comprehensive review. They concluded that while GHK-Cu does demonstrate anti-wrinkle effects in cellular studies, "there is a surprising absence of clinical studies using them." The review identified skin permeation as the central challenge: GHK's high aqueous solubility and low partition coefficient work against transdermal absorption. Metal complexation with copper and palmitoylation (creating Pal-GHK) both increase permeability, and cell-penetrating peptides and microneedle pretreatment show promise as enhancement strategies.[7]
The permeation challenge creates an important interpretive problem for the clinical data. If GHK-Cu penetrates poorly through intact skin, the observed clinical effects could be occurring primarily at the epidermal level rather than reaching dermal fibroblasts where collagen synthesis occurs. Alternatively, the copper ion may contribute independently of the peptide, or the clinical effects may be mediated through surface-level signaling that does not require deep penetration.
GHK-Cu versus other cosmetic peptides
Copper peptides in skincare have become a major product category, but GHK-Cu is one specific molecule within a broader family. Understanding where it fits among cosmetic peptides provides useful context.
Matrixyl (palmitoyl pentapeptide-4) targets the same collagen-stimulation endpoint but through a different mechanism and is five amino acids rather than three. GHK-Cu outperformed Matrixyl 3000 in the wrinkle volume comparison (31.6% additional reduction).[3]
Pal-GHK (palmitoyl-GHK) is a lipid-modified version of GHK designed for better skin penetration. By attaching a palmitic acid chain, the molecule gains lipophilicity and crosses the stratum corneum more readily. Many commercial "copper peptide" products actually contain Pal-GHK rather than GHK-Cu, but the two compounds have different physicochemical properties and may not behave identically in skin.
GHK-Cu stands apart from signal peptides (like argireline/acetyl hexapeptide-3) that work by modulating neurotransmitter release at the neuromuscular junction. GHK-Cu acts on extracellular matrix production and tissue remodeling, a fundamentally different mechanism. The practical implication is that GHK-Cu addresses structural skin aging (collagen loss, elasticity decline) while neurotransmitter-modulating peptides address dynamic wrinkles (expression lines).
Tripeptide-based wound healing research extends well beyond GHK-Cu. Arul et al. (2005) demonstrated that biotinylated GHK peptide incorporated into a collagenous matrix enhanced dermal wound healing in rat models, confirming that the GHK sequence retains biological activity when formulated into biomaterial scaffolds.[8]
The age-related decline and its implications
Age-Related Decline
GHK Blood Levels Drop 60% Between Age 20 and 60
Plasma GHK concentration (ng/mL) across the adult lifespan
60%
decline from age 20 to 60
120 ng/mL
lost over 40 years
Source: Dou et al. (2020), Aging Pathobiology and Therapeutics
 View as image
View as imageThe decline of circulating GHK from 200 ng/mL at age 20 to 80 ng/mL by age 60 correlates with reduced wound healing capacity, thinner skin, decreased collagen density, and slower tissue repair.[2] This correlation has led to the hypothesis that GHK depletion is not merely a marker of aging but a contributor to it, and that restoring GHK levels could partially reverse age-related tissue decline.
Pickart (2008) reviewed the broader tissue remodeling context and argued that GHK operates as a damage signal released from injured or aging tissue, recruiting repair processes that decline as the signal itself becomes less abundant.[4] The feedback loop model proposes: collagen degrades with age, releasing GHK fragments; GHK binds copper; GHK-Cu signals for new collagen and tissue repair; but declining GHK production means less signal and less repair with each passing decade.
This model is elegant but not fully proven. The correlation between declining GHK levels and declining skin quality does not establish causation. Other factors, including hormonal changes, UV cumulative damage, declining stem cell function, and altered immune function, contribute to skin aging independently of GHK levels.
Wound healing applications
GHK-Cu's original research context was wound healing, not cosmetics. The peptide accelerates wound closure in animal models including skin wounds, hair follicle regeneration, gastrointestinal tissue repair, bone tissue healing, and dog foot pad injuries.[3]
The wound healing data are more extensive than the cosmetic data and include systemic administration studies. Pickart and colleagues reported that systemic (injectable) GHK-Cu induced wound healing in rats, mice, and pigs, suggesting that the peptide's effects extend beyond the local application site.[3]
Nikolaeva et al. (2024) explored advanced delivery by evaluating GHK peptide-heparin interactions in multifunctional liposomal formulations, representing the frontier of GHK delivery technology where the peptide is packaged in lipid nanoparticles designed for controlled release and enhanced tissue penetration.[9]
For wound healing specifically, the evidence is stronger than for cosmetic anti-aging, because wound models involve measurable endpoints (wound closure rate, tissue tensile strength, histological analysis) in controlled animal studies. The transition from animal wound healing to human wound healing applications has not been systematically pursued in clinical trials, despite the preclinical evidence.
What the evidence does not show
No large, independent, placebo-controlled trials. The clinical studies cited for GHK-Cu on human skin are small, primarily industry-sponsored, and not registered in clinical trial databases. The 71-woman photoaging study lacks the methodological rigor expected for evidence-based dermatology claims. No independent research group has conducted a properly powered, double-blind, placebo-controlled trial of topical GHK-Cu for skin aging.
No identified receptor. Despite picomolar activity suggesting receptor-mediated signaling, the cellular receptor for GHK-Cu has not been identified. Without knowing the target, the mechanism of action remains incompletely understood, and it is not possible to optimize the peptide-receptor interaction or predict off-target effects.
Penetration remains the central challenge. Mortazavi et al. (2025) called the absence of clinical permeation data "surprising" given how widely GHK-Cu is marketed.[7] Whether topical products deliver sufficient GHK-Cu to the dermis is unresolved.
Loren Pickart's dual role. Much of the GHK-Cu literature comes from Loren Pickart, who both discovered the peptide and holds patents related to copper peptide skincare products. This is a conflict of interest that does not invalidate the research but requires independent confirmation, which has been limited.
Head-to-head data are sparse. The comparison to vitamin C and retinoic acid (70% vs 50% vs 40% collagen improvement) is cited widely but comes from a single study. Retinoids and vitamin C have decades of independent clinical evidence; GHK-Cu does not.
Safety
LowResearcher conflict of interest
Concern
Most GHK-Cu research comes from Loren Pickart, who discovered the peptide and holds patents for copper peptide skincare products. This is a structural conflict of interest. The research isn't invalid, but it needs independent confirmation that hasn't happened.
What the research says
GHK-Cu has a long commercial track record in skincare without reported safety concerns. The risk isn't that it's dangerous — it's that the efficacy claims may be inflated by non-independent research.
Particularly relevant for: Consumers evaluating copper peptide skincare purchases
What to do
GHK-Cu is likely safe for topical use. The open question is how well it works, not whether it's harmful. Look for products with published concentration data and realistic marketing claims.
Pickart conflict noted in Mortazavi et al. (2025)
Long-term safety and efficacy are unknown. Most clinical studies lasted 12 weeks. Whether GHK-Cu produces lasting skin changes, whether tolerance develops, and whether long-term copper exposure in skin has adverse effects are unanswered questions.
Researchers working on collagen peptides for joint health face similar challenges in demonstrating that orally consumed peptides reach their intended tissue targets at biologically active concentrations, a parallel problem to the topical delivery question for GHK-Cu.
The Bottom Line
GHK-Cu is a naturally occurring copper tripeptide that stimulates collagen synthesis at picomolar concentrations, modulates over 4,000 genes, and has shown measurable wrinkle reduction and collagen improvement in clinical studies. The biological evidence is robust at the cellular level, and clinical results are promising but limited by small study sizes, industry sponsorship, and absence of independent replication. Skin penetration remains the central unresolved question for topical products. The peptide's wound healing evidence is stronger than its cosmetic evidence, but neither has been validated through the rigorous clinical trials that established treatments like retinoids and vitamin C have undergone.
Sources & References
- 1RPEP-00080·Maquart, F X et al. (1988). “GHK-Cu Stimulated Collagen Production at Extremely Low Concentrations.” FEBS letters.Study breakdown →PubMed →↩
- 2RPEP-04782·Dou, Yan et al. (2020). “The potential of GHK as an anti-aging peptide..” Aging pathobiology and therapeutics.Study breakdown →PubMed →↩
- 3RPEP-02768·Pickart, Loren et al. (2015). “GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration..” BioMed research international.Study breakdown →PubMed →↩
- 4RPEP-01402·Pickart, Loren (2008). “GHK-Cu: The Complete Review of This Tissue Remodeling Tripeptide's Biology and Applications.” Journal of biomaterials science. Polymer edition.Study breakdown →PubMed →↩
- 5RPEP-03846·Pickart, Loren et al. (2018). “Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data..” Cosmetics.Study breakdown →PubMed →↩
- 6RPEP-04979·Ma, Wen-Hui et al. (2020). “GHK-Cu Peptide Reduces Lung Fibrosis and Inflammation in Mice by Blocking TGF-β Scarring Pathway.” Life sciences.Study breakdown →PubMed →↩
- 7RPEP-12644·Mortazavi, Seyedeh Maryam et al. (2025). “Topically applied GHK as an anti-wrinkle peptide: Advantages, problems and prospective..” BioImpacts : BI.Study breakdown →PubMed →↩
- 8RPEP-01007·Arul, V et al. (2005). “GHK Peptide in a Collagen Scaffold Accelerates Wound Healing in Rats.” Journal of biomedical materials research. Part B.Study breakdown →PubMed →↩
- 9RPEP-08959·Nikolaeva, Viktoriia et al. (2024). “Evaluation of GHK peptide-heparin interactions in multifunctional liposomal covering..” Journal of liposome research.Study breakdown →PubMed →↩