BPC-157 and TB-500 in Bodybuilding: The Evidence Gap
Peptides in Bodybuilding
87.5%
Of 16 patients reported significant pain improvement after intra-articular BPC-157 injection for chronic knee pain in the only published human musculoskeletal study.
Lee et al., Alternative Therapies in Health and Medicine, 2021
Lee et al., Alternative Therapies in Health and Medicine, 2021
If you only read one thing
BPC-157 and TB-500 are the two most popular healing peptides in bodybuilding. Rat studies consistently show BPC-157 speeds up tendon, muscle, and bone healing. TB-500 promotes cell migration and wound repair in animal models. But here's the reality check: BPC-157 has been tested in only about 18 human subjects total across all published studies, and TB-500 has zero human trials. The 'Wolverine stack' combining both rests on data from 4 patients with no placebo group. Both are WADA-banned and FDA-unapproved. The animal science is real, but anyone injecting these is part of an uncontrolled experiment.
Among the dozens of peptides circulating in bodybuilding culture, BPC-157 and TB-500 occupy a unique position. They are not used for muscle growth or fat loss. They are used for injury recovery, and they are frequently combined into what online communities call the "Wolverine stack." The name captures the aspiration: superhuman healing. For a broader view of how peptides are used in this subculture, see Peptides in Bodybuilding Culture: What's Used and Why.
The appeal is straightforward. Bodybuilders experience a high rate of musculoskeletal injuries from repetitive heavy loading. Conventional recovery timelines for tendon, ligament, and muscle tears can sideline training for months. BPC-157 and TB-500 promise to compress those timelines. The question is whether the evidence supports the promise, and the answer is more complicated than either advocates or critics typically acknowledge.
Key Takeaways
- Bodybuilders call the BPC-157 + TB-500 combo the "Wolverine stack" — it's supposed to speed healing of any injury.
- BPC-157 has been tested on about 18 humans total. TB-500 has zero human trials.
- The rat studies are real, but roughly half of all drugs that work in rats fail in people.
- The single human BPC-157 knee study had no placebo group — so the 87% success rate could just be placebo.
- Both peptides are banned by WADA — a positive test means sanctions regardless of intent.
- TB-500 is a 7-amino-acid fragment, but most animal studies used the full 43-amino-acid thymosin beta-4.
- Anyone injecting these is basically running an uncontrolled experiment on themselves.
BPC-157: What the Animal Data Actually Shows
BPC-157 (Body Protection Compound-157) is a synthetic pentadecapeptide derived from a sequence found in human gastric juice. It has never been isolated as a naturally occurring peptide at the doses used experimentally, but the parent protein BPC exists in gastric secretions.
The preclinical literature on BPC-157 for musculoskeletal healing is extensive. Gwyer et al. (2019) reviewed the evidence and found consistent acceleration of healing across multiple tissue types: tendons, muscles, ligaments, and bones in rat models.[1] The mechanisms proposed include enhanced angiogenesis (new blood vessel formation), upregulation of growth hormone receptor expression in tendon fibroblasts, modulation of nitric oxide pathways, and promotion of collagen synthesis.
Specific preclinical results that drive the bodybuilding narrative include:
Tendon healing. Staresinic et al. (2003) demonstrated that BPC-157 accelerated Achilles tendon healing in rats following complete transection. Treated animals showed earlier functional recovery and improved biomechanical properties of the repaired tendon compared to controls.[2]
Growth hormone receptor upregulation. Chang et al. (2014) showed that BPC-157 increased growth hormone receptor expression in tendon fibroblasts, suggesting a mechanism by which the peptide could amplify the body's own growth-factor-driven repair processes.[3] For bodybuilders already interested in growth hormone biology, this finding reinforced the perception that BPC-157 works through credible biological pathways.
Muscle crush injury. Novinscak et al. (2008) found that BPC-157 improved recovery from muscle crush injury in rats, with treated animals showing faster functional restoration and reduced inflammatory markers.[4]
These studies are methodologically sound within their scope. The limitation is not study quality but species translation. Rat tendons heal faster than human tendons at baseline, with different collagen composition, vascularity, and mechanical loading patterns. Rat metabolism processes peptides differently. Dosing that works in a 250-gram rat does not scale linearly to a 90-kilogram human. The bodybuilding community often cites the rat data as though the findings transfer directly, but preclinical positive results predict human efficacy roughly 50% of the time across drug development in general. Rat studies are hypothesis-generating, not proof of efficacy in humans.
The Thin Human Evidence for BPC-157
A 2025 systematic review by Vasireddi et al. in HSS Journal identified 36 studies on BPC-157 for orthopaedic applications. Of those, 35 were preclinical and only 1 was a published human clinical study.[5] McGuire et al. (2025) published a separate narrative review titled "Regeneration or Risk?" reaching a similar conclusion: the preclinical data is promising but the human evidence is almost nonexistent.[6]
The single published musculoskeletal human study, by Lee et al. (2021), reported outcomes from 16 patients who received intra-articular BPC-157 injections for various types of chronic knee pain. Of those treated with BPC-157 alone (12 patients), 91.6% reported significant pain improvement. When BPC-157 was combined with thymosin beta-4, 75% (3 of 4 patients) improved. Follow-up ranged from 6 months to 1 year, and benefits appeared sustained.[7]
These numbers are provocative but carry severe limitations. The study had no control group, no blinding, no randomization, and a sample size of 16. The placebo response rate for intra-articular injections in knee pain studies typically ranges from 30-50%, driven by the injection procedure itself, the clinical attention, and the natural fluctuation of chronic pain. Without a control arm, it is impossible to determine how much of the 87.5% response rate reflects BPC-157's pharmacological activity versus placebo effect plus natural disease course.
Lee et al. (2025) subsequently published a safety pilot examining intravenous infusion of BPC-157 in 2 healthy adults at doses up to 20 mg. No adverse effects were detected on biomarkers of heart, liver, kidney, thyroid, or blood glucose function.[8] Two subjects cannot establish safety; they can only fail to detect common acute toxicity. Rare adverse events require hundreds to thousands of participants to identify.
TB-500: Even Less Human Data
TB-500 is a synthetic peptide corresponding to the active region (amino acids 17-23) of thymosin beta-4, a 43-amino-acid protein involved in actin regulation, cell migration, and wound healing. Unlike BPC-157, which has at least some published human data, TB-500 has zero published human clinical trials.
The preclinical case for thymosin beta-4 is strong. Gonzalez-Franquesa et al. (2021) identified thymosin beta-4 as a human "exerkine," a factor secreted by contracting muscle cells. TMSB4X was the most upregulated secreted protein from contracting myotubes in proteomic analysis, and was acutely increased in the plasma of exercising humans regardless of insulin resistance status.[9] This finding provides a biological rationale for why bodybuilders gravitate toward TB-500: the body itself releases thymosin beta-4 during the kind of intense exercise that causes microtrauma.
In animal models, thymosin beta-4 has demonstrated wound healing acceleration (42% improvement in reepithelialization at 4 days), cardiac repair after myocardial infarction, corneal wound healing, and tendon tissue regeneration. Wu et al. (2020) developed electrospun thymosin beta-4-loaded nanofibers for tendon tissue engineering, showing enhanced tenocyte proliferation and tendon-specific gene expression in vitro.[10]
The gap between these preclinical findings and human evidence is total. One registered clinical trial (NCT00832091) examined thymosin beta-4 for venous stasis ulcers, a dermal wound healing application, not musculoskeletal repair. No results from that trial have been published in the peer-reviewed literature for sport or bodybuilding applications.
The distinction between thymosin beta-4 (the full 43-amino-acid protein) and TB-500 (the synthetic 7-amino-acid fragment) matters for interpreting the literature. Most published studies use full-length thymosin beta-4 or recombinant versions, not the TB-500 fragment that bodybuilders actually purchase. Whether the fragment replicates the full protein's biological activity in human tissues at the doses used recreationally is an untested assumption.
Head-to-Head
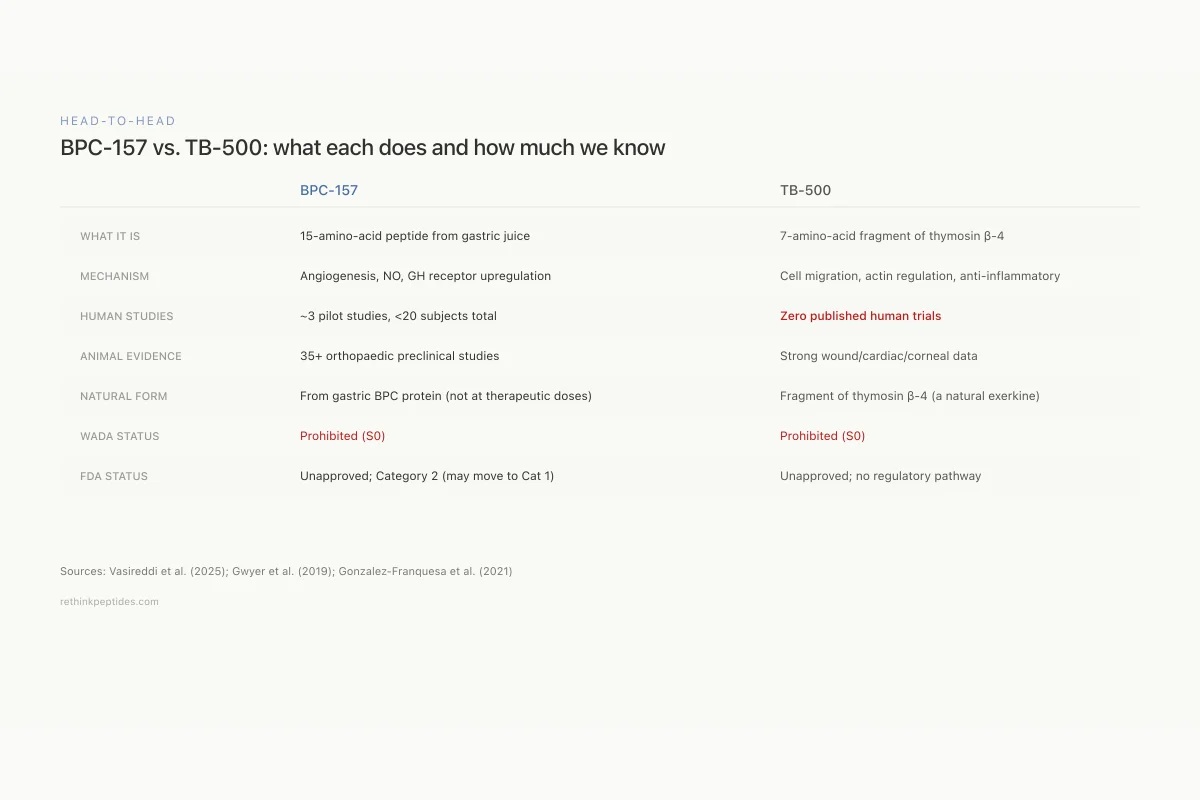
BPC-157 vs. TB-500: what each one does and how much we actually know
BPC-157
TB-500
What it is
Synthetic 15-amino-acid peptide from gastric juice sequence
Synthetic 7-amino-acid fragment of thymosin beta-4
Primary mechanism
Angiogenesis, NO modulation, GH receptor upregulation
Actin regulation, cell migration, anti-inflammatory
Tissue targets
Tendons, muscles, ligaments, gut lining
Wounds, cardiac tissue, cornea, tendons
Human studies
~3 pilot studies, <20 subjects total
Zero published human clinical trials
Animal evidence
35+ preclinical studies in orthopaedic contexts
Strong wound healing and cardiac repair data
Natural occurrence
Derived from gastric BPC protein; not isolated at therapeutic doses
Fragment of thymosin β-4, a natural exerkine released during exercise
WADA status
Prohibited (S0)
Prohibited (S0)
FDA status
Unapproved; Category 2 (may move to Cat 1)
Unapproved; no regulatory pathway active
What it is
BPC-157: Synthetic 15-amino-acid peptide from gastric juice sequence
TB-500: Synthetic 7-amino-acid fragment of thymosin beta-4
Primary mechanism
BPC-157: Angiogenesis, NO modulation, GH receptor upregulation
TB-500: Actin regulation, cell migration, anti-inflammatory
Tissue targets
BPC-157: Tendons, muscles, ligaments, gut lining
TB-500: Wounds, cardiac tissue, cornea, tendons
Human studies
BPC-157: ~3 pilot studies, <20 subjects total
TB-500: Zero published human clinical trials
Animal evidence
BPC-157: 35+ preclinical studies in orthopaedic contexts
TB-500: Strong wound healing and cardiac repair data
Natural occurrence
BPC-157: Derived from gastric BPC protein; not isolated at therapeutic doses
TB-500: Fragment of thymosin β-4, a natural exerkine released during exercise
WADA status
BPC-157: Prohibited (S0)
TB-500: Prohibited (S0)
FDA status
BPC-157: Unapproved; Category 2 (may move to Cat 1)
TB-500: Unapproved; no regulatory pathway active
Sources: Vasireddi et al. (2025); Gwyer et al. (2019); Gonzalez-Franquesa et al. (2021)
 View as image
View as imageThe "Wolverine Stack": Combining BPC-157 and TB-500
The combination of BPC-157 and TB-500 is the most popular peptide protocol in bodybuilding injury recovery forums. The logic behind stacking them is that BPC-157 acts primarily through angiogenesis, nitric oxide modulation, and growth factor receptor upregulation, while TB-500 acts through actin polymerization, cell migration, and anti-inflammatory signaling. In theory, they target complementary healing pathways.
Lee et al. (2021) included 4 patients who received the combination, with 75% (3 of 4) reporting improvement.[7] This is the only published human data on the combination, and 4 patients without controls produces no meaningful statistical signal.
Mayfield et al. (2026) published a primer on injectable peptide therapy for orthopaedic and sports medicine physicians, acknowledging the growing clinical interest while emphasizing the absence of Phase II or Phase III trial data for either peptide alone or in combination.[11] Rahman et al. (2026) reviewed therapeutic peptides in orthopaedics more broadly, positioning BPC-157 and thymosin beta-4 as promising candidates that require controlled clinical validation before evidence-based use can be supported.[12]
What Bodybuilders Don't Know: Regulatory and Detection Reality
Both BPC-157 and TB-500 are prohibited by the World Anti-Doping Agency (WADA) under the category S0 (non-approved substances). Neither has FDA approval for any indication. Their presence in a competitive athlete's sample constitutes a doping violation regardless of the reason for use.
Anti-doping laboratories can detect both peptides. Ho et al. (2012) validated a liquid chromatography-mass spectrometry method for detecting TB-500 in urine and plasma, establishing that the synthetic peptide can be distinguished from endogenous thymosin beta-4 fragments.[13] Cox et al. (2017) developed methods for detecting BPC-157 and its metabolites, demonstrating that the peptide is identifiable even after partial in vivo degradation.[14]
For bodybuilders competing in tested federations, using either peptide is a disqualification risk. For recreational bodybuilders, the legal status is less clear: BPC-157 and TB-500 occupy a gray market where they are sold "for research purposes only." The quality, purity, and actual content of gray-market peptides is unregulated and variable. Independent testing of online peptide products has found contamination, under-dosing, and mislabeling. A bodybuilder injecting a product labeled "BPC-157" or "TB-500" has no guarantee of receiving the correct peptide at the stated concentration, in a sterile formulation, free of endotoxins or degradation products.
Safety
ModerateGray-market peptide quality is unverified
Concern
BPC-157 and TB-500 purchased online are unregulated. Independent testing of gray-market peptides has found contamination, under-dosing, and mislabeling. A bodybuilder injecting a product labeled 'BPC-157' has no guarantee of receiving the correct peptide, at the stated dose, in a sterile formulation.
What the research says
Neither peptide is available through regulated pharmacies. The 2026 FDA reclassification may move BPC-157 to Category 1, enabling compounding pharmacies to prepare it under medical oversight — but this hasn't happened yet.
Particularly relevant for: Anyone self-administering BPC-157 or TB-500 from online 'research chemical' vendors
What to do
If you choose to use these peptides, understand you're injecting an unverified product. At minimum, use vendors who provide third-party certificate of analysis from an independent lab (not the manufacturer), and never share injection supplies.
FDA enforcement records; Vasireddi et al. (2025)
The injury prevention question also intersects with the health risks of peptide use in bodybuilding. BPC-157's pro-angiogenic mechanism, the same property that theoretically aids healing, raises questions about whether chronic use could promote tumor vascularization in individuals with undetected malignancies.
What Would Adequate Evidence Look Like?
The gap between the current evidence and what would be needed to validate BPC-157 and TB-500 for injury recovery is substantial:
For BPC-157: A randomized, double-blind, placebo-controlled trial in at least 100-200 patients with a defined musculoskeletal injury (e.g., partial rotator cuff tear, patellar tendinopathy), using standardized doses, validated outcome measures, and follow-up of at least 12 months. No such trial has been completed or, to public knowledge, registered.
For TB-500: The same, but starting from an even earlier position since there are no published human musculoskeletal data at all.
For the combination: An additional arm comparing BPC-157 alone, TB-500 alone, the combination, and placebo would be needed to determine whether stacking adds benefit over either peptide individually. This four-arm design would require at least 400-800 participants and millions in funding, which explains why no pharmaceutical company or academic center has undertaken it for peptides that cannot be patented.
The economic reality is that BPC-157 and TB-500 are unpatentable sequences. Without patent protection, no company can recoup the $50-100 million investment required for Phase II and Phase III trials. This is why the gray market, not traditional drug development, has driven adoption. The bodybuilding community functions as a de facto uncontrolled trial population.
Until controlled trials exist, the bodybuilding community's use of BPC-157 and TB-500 represents a large-scale uncontrolled experiment. Individual reports of success circulate widely on forums and social media, but without controls, these anecdotes cannot distinguish drug effect from placebo response, natural healing, concurrent treatments, or reporting bias. The peptides may work. They may not. The honest answer is that the evidence is insufficient to know. For related context on GH-stimulating peptides popular in the same communities, see GH Peptides for Body Composition: Separating Gym Lore from Evidence.
The Bottom Line
BPC-157 has consistent preclinical evidence for musculoskeletal healing acceleration in rat models, but only one published uncontrolled human study (16 patients, no placebo group). TB-500 has zero published human musculoskeletal data despite strong preclinical wound healing evidence. The "Wolverine stack" combining both peptides rests on 4 patients without controls. Both peptides are WADA-prohibited and FDA-unapproved. The gap between the preclinical promise and clinical evidence remains one of the widest in peptide therapeutics. For a deeper look at BPC-157 specifically, see BPC-157: The Body Protection Compound and What the Research Shows.
Sources & References
- 1RPEP-04213·Gwyer, Daniel et al. (2019). “BPC-157 for Tendon, Ligament, and Muscle Healing: What the Animal Research Shows.” Cell and tissue research.Study breakdown →PubMed →↩
- 2RPEP-00860·Staresinic, M et al. (2003). “BPC-157 Accelerates Achilles Tendon Healing and Directly Stimulates Tendon Cell Growth.” Journal of orthopaedic research : official publication of the Orthopaedic Research Society.Study breakdown →PubMed →↩
- 3RPEP-02350·Chang, Chung-Hsun et al. (2014). “Pentadecapeptide BPC 157 enhances the growth hormone receptor expression in tendon fibroblasts..” Molecules (Basel.Study breakdown →PubMed →↩
- 4RPEP-01394·Novinscak, Tomislav et al. (2008). “BPC-157 Heals Muscle Crush Injury in Rats.” Surgery today.Study breakdown →PubMed →↩
- 5RPEP-13892·Vasireddi, Nikhil et al. (2025). “BPC-157 for Sports Injuries: What a Systematic Review of the Evidence Actually Shows.” HSS journal : the musculoskeletal journal of Hospital for Special Surgery.Study breakdown →PubMed →↩
- 6RPEP-12503·McGuire, Flynn P et al. (2025). “BPC-157 for Muscle and Tendon Healing: What Science Actually Shows vs. What Athletes Believe.” Current reviews in musculoskeletal medicine.Study breakdown →PubMed →↩
- 7RPEP-05534·Lee, Edwin et al. (2021). “BPC-157 Knee Injections Relieved Pain in 88% of Patients Across Multiple Knee Conditions.” Alternative therapies in health and medicine.Study breakdown →PubMed →↩
- 8RPEP-12011·Lee, Edwin et al. (2025). “First Study of Intravenous BPC-157 in Humans Shows No Side Effects in Two Patients.” Alternative therapies in health and medicine.Study breakdown →PubMed →↩
- 9RPEP-05412·Gonzalez-Franquesa, Alba et al. (2021). “Thymosin Beta-4 Is a Key Exercise-Released Peptide That Acts as a Growth Factor.” American journal of physiology. Cell physiology.Study breakdown →PubMed →↩
- 10RPEP-05204·Wu, Shaohua et al. (2020). “Thymosin Beta-4 Loaded Nanofiber Yarns Show Promise for Tendon Tissue Engineering.” Materials science & engineering. C.Study breakdown →PubMed →↩
- 11RPEP-15687·Mayfield, Cory K et al. (2026). “Injectable Peptide Therapy: A Primer for Orthopaedic and Sports Medicine Physicians..” The American journal of sports medicine.Study breakdown →PubMed →↩
- 12RPEP-15961·Rahman, Omar F et al. (2026). “Therapeutic Peptides in Orthopaedics: Applications, Challenges, and Future Directions..” Journal of the American Academy of Orthopaedic Surgeons. Global research & reviews.Study breakdown →PubMed →↩
- 14RPEP-03254·Cox, Holly D et al. (2017). “Detection and in vitro metabolism of the confiscated peptides BPC 157 and MGF R23H..” Drug testing and analysis.Study breakdown →PubMed →↩