Body Image After GLP-1 Weight Loss: What Changes
GLP-1 and Psychology
71% of GLP-1-Interested Participants Were Women
In a 2025 Body Image study of 225 university participants, interest in GLP-1 weight loss medications was significantly predicted by body shame, body surveillance, weight concerns, and lower body appreciation, independent of actual BMI.
Markey et al., Body Image, 2025
Markey et al., Body Image, 2025
If you only read one thing
Losing 20-30% of your body weight from Ozempic or Mounjaro is a bigger psychological change than most people expect. Many patients feel better — less depressed, less anxious, more in control of food. But rapid weight loss also brings challenges your brain wasn't ready for: 'phantom fat' (where you still see your old body when you look in the mirror), identity lag (your sense of self doesn't match your new body), excess skin that won't retract, and a potential crisis if you stop the medication and the weight comes back. Interest in these drugs is driven more by body shame than by actual BMI — which means weight loss alone may not fix the dissatisfaction. The medication is the easy part; rebuilding your self-image around a new body takes much longer.
Semaglutide and tirzepatide produce weight losses of 15 to 25% of body weight in clinical trials, magnitudes previously seen only after bariatric surgery. For someone weighing 120 kg, that is 18 to 30 kg lost over 68 to 72 weeks. The physical transformation is visible, measurable, and often dramatic. The psychological transformation is less predictable. Some people experience improved self-esteem, reduced depression, and better quality of life. Others find that losing the weight does not resolve the body dissatisfaction that motivated them to seek treatment. Some develop new psychological challenges: phantom fat perception, identity confusion, excess skin distress, and a complicated relationship with a body that changed faster than their self-concept could follow. The research on body image after GLP-1-mediated weight loss is still emerging, but early findings reveal patterns that clinicians and patients should understand before starting treatment.
Key Takeaways
- Body shame, body surveillance, and weight concerns predicted interest in GLP-1 medications independently of BMI, while body appreciation served as a protective factor reducing interest in weight loss drugs (Markey et al., Body Image, 2025)
- In adults with Class 3 obesity, 12 months of GLP-1 RA therapy was associated with reduced eating disorder risk scores and decreased psychological distress (Maynard et al., International Journal of Eating Disorders, 2026)
- A systematic review of psychiatric effects found modest antidepressant effects of GLP-1 RAs, inconsistent associations with suicidality, and potential therapeutic benefits for substance use disorders (Sa et al., Diabetes, Obesity and Metabolism, 2026)
- Qualitative interviews with adults on semaglutide and tirzepatide revealed a central theme of "taking back control" over food behaviors, body, and healthcare interactions (Trocchio et al., Obesity Pillars, 2026)
- A large cohort study of 51,803 patients found GLP-1 RA users had significantly lower risk of depression (HR 0.73) and anxiety (HR 0.77) compared to matched controls, with no increased suicidal behavior (Kornelius et al., Scientific Reports, 2024)
- Weight loss plateau after semaglutide occurs at approximately 60 to 68 weeks; body contouring surgery should wait until weight has stabilized for at least 3 to 6 months (Garbaccio et al., Aesthetic Plastic Surgery, 2025)
Who Seeks GLP-1 Medications and Why
The psychological profile of people seeking GLP-1 weight loss drugs is not simply "people who weigh more." Markey et al. (2025) studied 225 university participants and found that interest in GLP-1 medications was driven by body image variables more than by objective weight status.[1]
Specifically, higher body shame, greater body surveillance (habitually monitoring one's appearance), and more intense weight concerns all independently predicted interest in GLP-1 drugs. BMI was also a predictor, but body image dissatisfaction added predictive power beyond weight alone. Crucially, body appreciation, defined as feeling respectful, grateful, or compassionate toward one's body, served as a protective factor. Participants with high body appreciation were less interested in weight loss medications even when they reported weight concerns, suggesting that the relationship with one's body matters as much as the body itself.
Who Wants GLP-1 Medications and Why
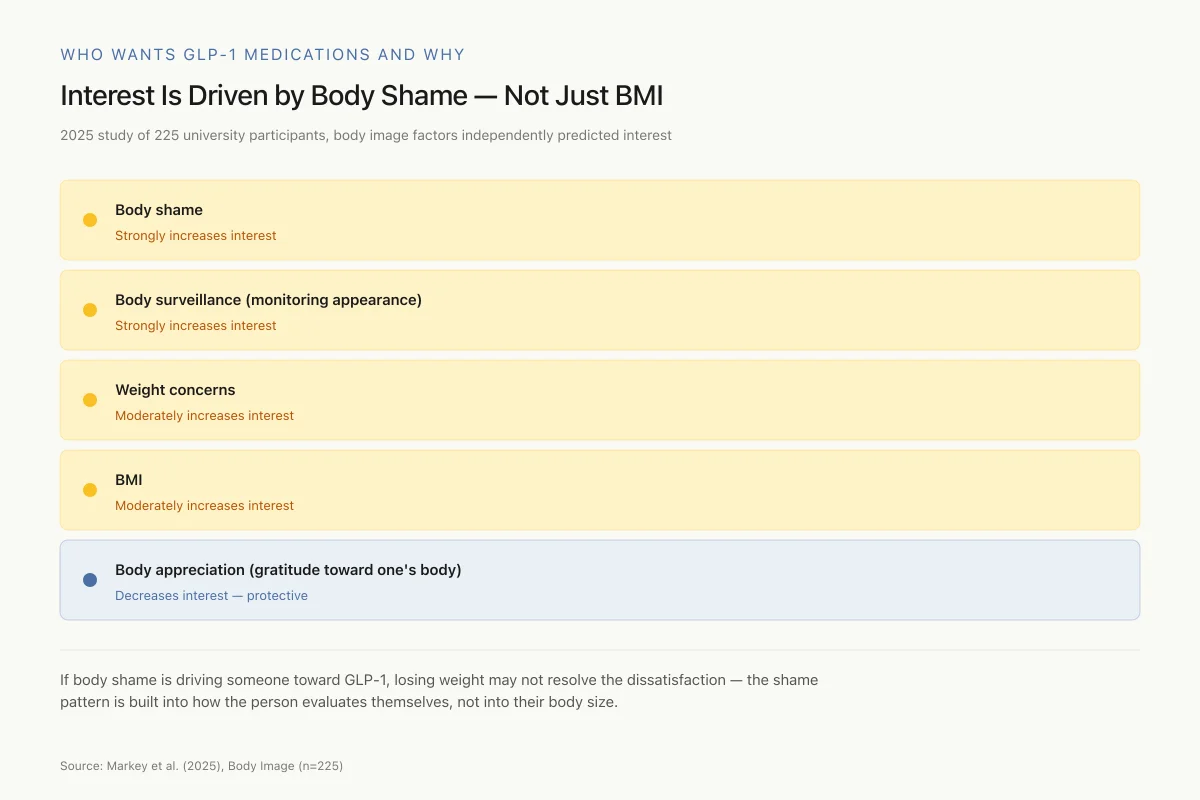
Interest Is Driven by Body Shame — Not Just BMI
A 2025 study of 225 university participants found body image factors independently predicted interest in weight-loss drugs
If body shame is driving someone toward GLP-1 medication, losing weight may not resolve the dissatisfaction — the shame pattern is built into how the person evaluates themselves, not into their body size. This is why some patients achieve the target weight but still feel the same about their body.
Source: Markey et al. (2025), Body Image (n=225)
 View as image
View as imageThis finding has implications for predicting who will be psychologically satisfied after GLP-1-mediated weight loss. If the motivation for seeking treatment is body shame rather than health, achieving a lower weight may not resolve the underlying dissatisfaction. Body shame is a cognitive and emotional pattern rooted in internalized social messages, personal history, and self-evaluation frameworks, not a simple response to body size. The pattern often begins in childhood or adolescence and solidifies over decades. People who approach weight loss medications expecting their body image to improve proportionally to their weight loss may be disappointed. The assumption that "if I weigh less, I will feel better about my body" is intuitive but not consistently supported by the evidence. Many people who lose substantial weight discover that the body dissatisfaction migrates rather than disappears: attention shifts from overall size to specific areas, to skin quality, to the speed of remaining weight loss, to comparison with an idealized outcome that the medication cannot deliver.
The Eating Disorder Question
One of the earliest psychological concerns raised about GLP-1 medications was whether they might trigger or worsen eating disorders. The drugs profoundly alter appetite, reduce food preoccupation (the "food noise" phenomenon), and can produce rapid weight loss, all factors that intersect with eating disorder psychopathology. For a focused analysis of this risk, see Can GLP-1 Drugs Trigger Eating Disorders? What Clinicians Are Watching.
Maynard et al. (2026) provided the first substantial longitudinal data, studying adults with Class 3 obesity (BMI 40 or higher) in a multidisciplinary weight management program.[2] Participants who initiated GLP-1 RA therapy were assessed at baseline and 12 months using the Eating Disorder Examination-Questionnaire Short (EDE-QS) and the Kessler Psychological Distress Scale (K10). At 12 months, eating disorder risk scores had decreased and psychological distress had improved. The direction of these findings is reassuring: in this clinical population, GLP-1 therapy was associated with reduced, not increased, eating disorder symptomatology.
Krug et al. (2025) offered a more nuanced perspective in a narrative review synthesizing evidence on GLP-1 usage in the context of eating disorders and psychosocial processes.[3] They noted that GLP-1 RAs influence appetite and reward pathways in ways that could either help or harm depending on the individual's eating disorder profile. For binge eating disorder, reduced appetite and diminished food reward may be beneficial. For restrictive eating disorders, the same effects could reinforce pathological restriction. The review emphasized the need for individualized psychiatric assessment before and during GLP-1 treatment, particularly in patients with eating disorder histories.
Phantom Fat and Identity Lag
Clinicians working with post-weight-loss patients consistently describe a phenomenon variously called "phantom fat," "ghost fat," or "vestigial body image": patients who have lost substantial weight continue to perceive themselves as their former size. They reach for larger clothing sizes. They avoid narrow spaces they could now fit through. They do not recognize the person in photographs.
This is not body dysmorphic disorder in the clinical sense, though it shares features. It is better understood as an identity lag: the internalized body schema, built over years or decades of living in a larger body, updates more slowly than the actual body changes. The brain maintains an internal representation of body size and shape that informs spatial navigation, clothing selection, social behavior, and self-perception. This representation is updated through proprioceptive feedback and visual self-recognition, but the update process is gradual.
A 2018 study published in Clinical Nursing found that many women could not recognize or accept their new bodies even 18 to 30 months after bariatric surgery. Some patients reported feeling fraudulent in their new body, as though they were pretending to be someone they were not. Others described anxiety about social interactions because they no longer knew how to present themselves. The weight was gone, but the psychological architecture built around it remained.
The GLP-1 era may intensify this phenomenon because the weight loss can be faster and more dramatic than traditional interventions, giving the psychological self even less time to adapt. Bariatric surgery patients typically lose weight rapidly in the first 6 months, then gradually over the next 12 to 18 months. GLP-1 medications can produce sustained, near-linear weight loss for over 60 weeks. The cumulative effect is similar, but the sustained pace may prevent the psychological processing that happens during plateaus.
For patients with histories of weight-based stigma, bullying, or discrimination, the identity shift is particularly complex. Losing the body that defined their social experiences can feel like losing part of their history. Some patients report that others treat them differently after weight loss, and the contrast between past and present social interactions can trigger grief, anger, or confusion about which version of themselves is "real."
The Psychological Aftermath
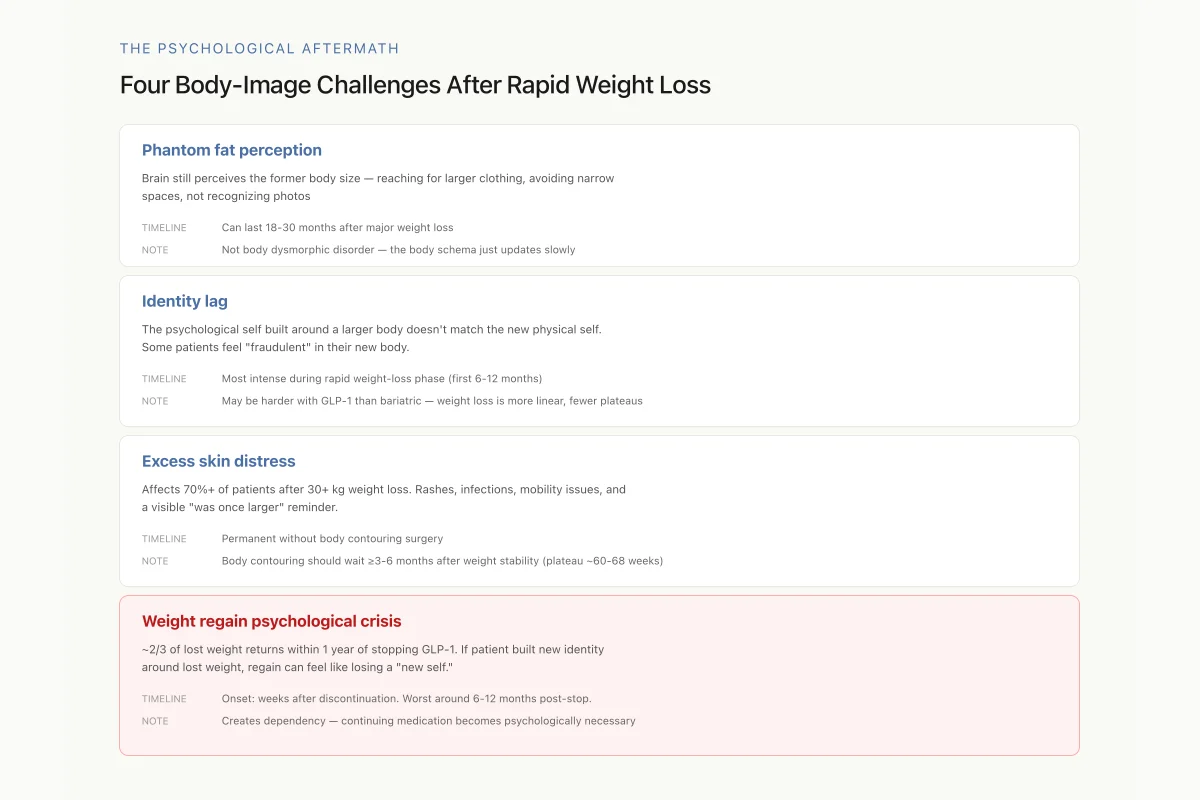
Four Body-Image Challenges That Can Show Up After Rapid Weight Loss
Weight loss medications are designed around body composition, not body perception. A successful drug outcome (20%+ weight loss) can coexist with any of these four unresolved psychological challenges — which is why clinical guidelines increasingly recommend psychological screening alongside GLP-1 prescription.
Source: Trocchio et al. (2026); Garbaccio et al. (2025); qualitative body-image literature
 View as image
View as imageThe qualitative study by Trocchio et al. (2026) captured this dynamic from the patient perspective.[4] Adults using semaglutide and tirzepatide for obesity treatment described their experience through a central theme of "taking back control" over food behaviors, their bodies, and their healthcare interactions. This framing is psychologically significant: it positions the medication as restoring agency rather than creating passive dependence. Participants described reduced food preoccupation, better ability to make intentional food choices, and improved confidence in medical encounters. For more on the food noise phenomenon, see What Is "Food Noise" and How Do GLP-1 Drugs Quiet It?.
Depression, Anxiety, and GLP-1 Treatment
The psychiatric effects of GLP-1 medications extend beyond body image into broader mental health outcomes. Sa et al. (2026) conducted a systematic review of the emerging evidence on GLP-1 RA psychiatric effects.[5] Their findings revealed a complex picture: modest antidepressant effects in most studies, inconsistent associations with suicidality, potential therapeutic benefits for substance use disorders, and emerging evidence for effects on schizophrenia spectrum disorders.
The largest cohort study to date, by Kornelius et al. (2024), analyzed 51,803 patients with obesity prescribed GLP-1 RAs compared to matched controls.[6] GLP-1 RA users had a 27% lower risk of depression (hazard ratio 0.73) and a 23% lower risk of anxiety (hazard ratio 0.77) compared to non-users. No increased risk of suicidal behavior was detected. These protective effects persisted across subgroups and sensitivity analyses.
A 2026 randomized clinical trial went further, testing semaglutide specifically for cognitive dysfunction in patients with major depressive disorder (MDD).[7] This study, published in Med, represents the first RCT of a GLP-1 RA for a primary psychiatric indication rather than obesity. The trial tested whether semaglutide could improve cognitive symptoms in depression, reflecting growing recognition that GLP-1 receptors in the brain may have direct neuropsychiatric effects independent of weight loss.
Two Different Signals
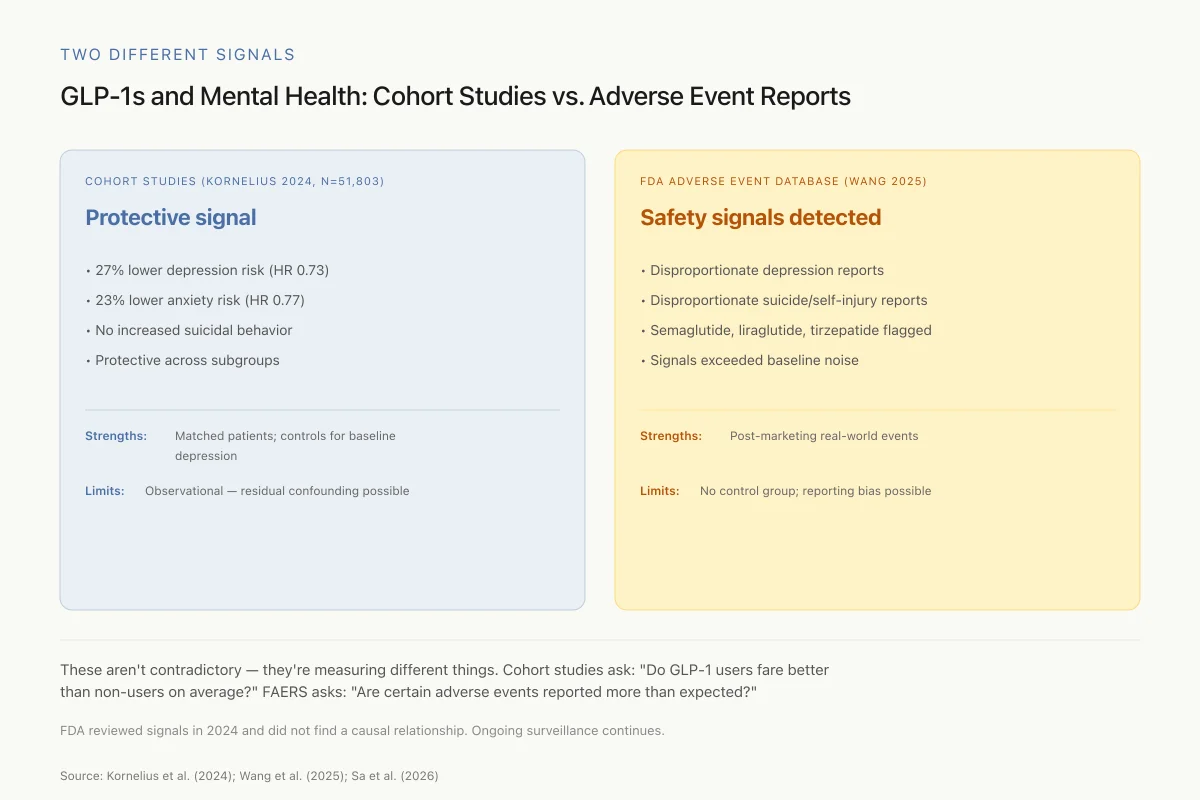
GLP-1s and Mental Health: Cohort Studies vs. Adverse Event Reports
The two main sources of psychiatric safety data point in opposite directions — here's why
These aren't contradictory — they're measuring different things. Cohort studies answer: "On average, across the full population, do GLP-1 users fare better than non-users?" FAERS answers: "Are certain adverse events being reported more than expected?" Both types of evidence matter. The FDA reviewed the signals in 2024 and did not find a causal relationship, but ongoing surveillance continues.
Source: Kornelius et al. (2024); Wang et al. (2025); Sa et al. (2026) systematic review
 View as image
View as imageHowever, not all data is reassuring. Wang et al. (2025) conducted a disproportionality analysis of the FDA Adverse Event Reporting System (FAERS) database, finding signals for depression and suicide/self-injury associated with semaglutide, liraglutide, and tirzepatide.[8] FAERS analyses detect signals, not causal relationships; reporting biases and media attention can inflate signal detection. But the signals warrant ongoing surveillance, particularly as GLP-1 prescriptions expand into populations without diabetes where the risk-benefit calculus differs. For the FDA investigation and its conclusions, see GLP-1 Drugs and Suicidal Thoughts: What the FDA Investigation Found. For a deeper analysis of the depression evidence, see Semaglutide and Depression: Does Weight Loss Help or Hurt Mental Health?.
A retrospective chart review by Sa et al. (2026) documented psychiatric manifestations in clinical practice, providing real-world data to complement the controlled trial evidence.[9]
Excess Skin and Body Contouring
For patients who lose 30 kg or more, excess skin is not a cosmetic inconvenience; it is a physical and psychological burden. Skin that stretched to accommodate the larger body does not retract fully, leaving folds that can cause rashes, infections, mobility limitations, and profound body dissatisfaction. Studies of post-bariatric surgery patients consistently find that excess skin is one of the strongest predictors of poor body image despite successful weight loss. The same pattern is emerging in the GLP-1 population.
Garbaccio et al. (2025) conducted a systematic review of timing considerations for body contouring surgery after semaglutide-associated weight loss.[10] They found that weight loss plateau after semaglutide occurs at approximately 60 to 68 weeks, similar to the 12- to 18-month stabilization window after bariatric surgery. They recommended that body contouring surgery wait until weight has been stable for at least 3 to 6 months after plateau. A complicating factor is weight recurrence after GLP-1 discontinuation: if patients stop semaglutide, they typically regain two-thirds of lost weight within one year, which would distort body contouring outcomes. Surgical timing must account for whether the patient plans to continue medication indefinitely.
Abbott et al. (2026) compared complication rates for body contouring surgery across weight loss modalities: bariatric surgery, GLP-1 pharmacotherapy, combination therapy, and lifestyle modification.[11] This study provides the first comparative data on surgical outcomes across the different weight loss pathways, informing the growing number of patients seeking body contouring after GLP-1-mediated weight loss.
The demand for body contouring after GLP-1 weight loss is creating a new surgical population. Unlike post-bariatric patients who have undergone a major surgical procedure and are typically followed closely by a bariatric team, GLP-1 patients may have lost comparable amounts of weight through a prescription obtained from a primary care physician or telehealth visit. They may not have the multidisciplinary support structure that bariatric programs provide, including psychological screening. Plastic surgeons are encountering patients with unrealistic expectations about what body contouring can achieve, patients who expect surgery to complete a transformation that the GLP-1 medication started. When the surgical result reveals not the idealized body they imagined but an improved version of the real body they have, disappointment can follow.
The psychological burden of excess skin is often underestimated. For many patients, the skin folds become a visible reminder that their body was once much larger, undermining the sense of transformation they felt during active weight loss. In situations where insurance does not cover body contouring (classified as cosmetic rather than reconstructive in many health systems), the financial barrier adds frustration. Patients may feel they have done the work of losing the weight but cannot complete the process.
The Alcohol and Substance Use Connection
An unexpected psychological dimension of GLP-1 treatment is reduced interest in alcohol. Many patients report spontaneously drinking less or losing interest in alcohol entirely while on semaglutide or tirzepatide. The systematic review by Sa et al. (2026) identified emerging evidence that GLP-1 RAs may have therapeutic effects in substance use disorders, potentially through modulation of reward pathways that overlap between food and substance consumption.[5] For a focused analysis of this phenomenon, see GLP-1 Agonists and Alcohol: Why Some People Lose Interest in Drinking.
What the Evidence Does and Does Not Support
The body image picture after GLP-1 weight loss is more complicated than "lose weight, feel better." The evidence supports several conclusions and raises several uncertainties:
Supported by evidence: GLP-1 RAs reduce eating disorder symptomatology in people with Class 3 obesity over 12 months. Large cohort data shows reduced depression and anxiety risk. Patients report a sense of regained control over food behaviors.
Mixed evidence: The relationship between weight loss magnitude and body image improvement is not linear. Phantom fat perception and identity lag affect an unknown proportion of patients. FAERS signals for depression and suicidality exist alongside cohort data showing protective effects.
Not established: Whether body image satisfaction improves proportionally to weight loss. Whether patients with pre-existing body dysmorphic tendencies do better or worse on GLP-1 therapy. The long-term psychological effects of medication-dependent weight maintenance. Whether stopping GLP-1 medications and regaining weight causes worse psychological outcomes than never having lost weight.
Unknown but clinically important: How trauma histories interact with rapid weight loss. Whether patients who seek GLP-1 medications primarily from body shame rather than health motivation experience different psychological trajectories. What psychological support structures improve long-term outcomes after GLP-1-mediated weight loss. Whether the weight regain that typically follows GLP-1 discontinuation produces worse psychological outcomes than the original obesity.
Safety
ModerateWeight regain after stopping GLP-1s can cause a psychological crisis
Concern
Two-thirds of lost weight typically returns within a year of stopping semaglutide. For patients who built a new identity, wardrobe, and social presentation around the lost weight — and possibly had body contouring surgery — regain isn't just a physical setback. It can feel like losing a 'new self.'
What the research says
Discuss long-term medication strategy before starting. If you might need to stop (cost, side effects, life circumstances), build psychological support in advance. 'Continue indefinitely' is a real decision, not just a default.
Particularly relevant for: Anyone starting GLP-1 therapy who has invested significant identity in weight loss
What to do
Before stopping, discuss tapering strategies with your prescriber, maintain therapeutic support through the transition, and be prepared for the possibility of regain. Regaining is not a personal failure — it's the pharmacology.
Garbaccio et al. (2025); weight regain literature after GLP-1 discontinuation
The weight regain question deserves special attention. Two-thirds of lost weight typically returns within one year of stopping semaglutide. For patients who have psychologically adapted to their new body, rebuilt their wardrobe, changed their social presentation, and perhaps invested in body contouring surgery, regaining that weight represents not just a physical setback but a potential psychological crisis. The experience of losing a "new self" may be more distressing than never having lost weight in the first place. This creates a dependency dynamic where continuing GLP-1 medication becomes psychologically necessary to maintain not just weight but identity. No longitudinal data yet tracks the psychological trajectory of GLP-1 discontinuation and weight regain.
The GLP-1 era is producing weight losses at a pace and scale that outstrip our psychological understanding of how people adapt to dramatically changed bodies. The biological science of these drugs is advanced; the psychological science is just beginning. For an overview of how GLP-1 medications connect to the broader peptide research landscape, see Autoimmune Diabetes and GLP-1: What the Research Suggests.
The Bottom Line
GLP-1 medications produce rapid, substantial weight loss that creates genuine psychological adjustment challenges alongside physical transformation. The evidence shows that body image dissatisfaction, not just excess weight, drives interest in these medications. In clinical populations, GLP-1 therapy appears to reduce eating disorder risk and psychological distress over 12 months. Large cohort data shows reduced depression and anxiety risk. Qualitative research reveals patients experiencing restored agency over food and body. But complications exist: phantom fat perception, identity lag, excess skin distress, and FAERS signals for depression and suicidality that warrant ongoing surveillance. The gap between the biological science of GLP-1 drugs and the psychological science of living in a rapidly changing body remains wide and needs closing.
Sources & References
- 1RPEP-12450·Markey, Charlotte H et al. (2025). “Body image and interest in GLP-1 weight loss medications..” Body image.Study breakdown →PubMed →↩
- 2RPEP-15688·Maynard, Sian et al. (2026). “Effects of GLP-1 Receptor Agonist Therapy on Eating Disorder Risk and Psychological Distress in Adults With Class 3 Obesity..” The International journal of eating disorders.Study breakdown →PubMed →↩
- 3RPEP-11932·Krug, Isabel et al. (2025). “Beyond Weight Loss: GLP-1 Usage and Appetite Regulation in the Context of Eating Disorders and Psychosocial Processes..” Nutrients.Study breakdown →PubMed →↩
- 4RPEP-16276·Trocchio, Lauren Lynn et al. (2026). “Taking back control: The experience of adults using semaglutide and tirzepatide for obesity treatment - A qualitative study..” Obesity pillars.Study breakdown →PubMed →↩
- 5RPEP-16030·Sa, Brianna et al. (2026). “Do GLP-1 Drugs Affect Mental Health? A Systematic Review of Psychiatric Effects.” Diabetes.Study breakdown →PubMed →↩
- 6RPEP-08587·Kornelius, Edy et al. (2024). “The risk of depression, anxiety, and suicidal behavior in patients with obesity on glucagon like peptide-1 receptor agonist therapy..” Scientific reports.Study breakdown →PubMed →↩
- 7RPEP-14811·Badulescu, Sebastian et al. (2026). “Semaglutide Improves Cognitive Function in People with Depression and Obesity.” Med (New York.Study breakdown →PubMed →↩
- 8RPEP-14027·Wang, Min et al. (2025). “Depression and suicide/self-injury signals for weight loss medications: A disproportionality analysis of semaglutide, liraglutide, and tirzepatide in FAERS database..” Journal of affective disorders.Study breakdown →PubMed →↩
- 9RPEP-16031·Sa, Brianna et al. (2026). “Retrospective chart review on psychiatric manifestations of GLP-1 agonist usage..” Journal of psychiatric research.Study breakdown →PubMed →↩
- 10RPEP-11043·Garbaccio, Noelle C et al. (2025). “When to Get Body Contouring Surgery After Semaglutide Weight Loss — and Why Weight Regain Is a Concern.” Aesthetic plastic surgery.Study breakdown →PubMed →↩
- 11RPEP-14688·Abbott, Erin N et al. (2026). “Body Contouring Surgery After GLP-1 Weight Loss Has Similar Complication Rates to Other Methods.” Aesthetic surgery journal.Study breakdown →PubMed →↩