Retatrutide: The Triple Agonist for Weight Loss
Retatrutide
28.7%
In the first phase 3 trial (TRIUMPH-4), retatrutide 12 mg produced 28.7% mean body weight reduction at 68 weeks, translating to an average loss of 71.2 lbs.
Eli Lilly, TRIUMPH-4 Phase 3 Results, December 2025
Eli Lilly, TRIUMPH-4 Phase 3 Results, December 2025
If you only read one thing
Retatrutide is the next-generation weight loss shot from Eli Lilly. It hits three hormone targets at once — GLP-1 (like Ozempic), GIP (like Mounjaro), and glucagon (new). In its first phase 3 trial, people lost 28.7% of their body weight over 68 weeks — about 71 pounds on average. That's the biggest number from any weight loss drug trial ever run. But it comes with more side effects than the currently approved options: about 18% of people quit the highest dose because of them, and a new side effect (abnormal skin sensations) showed up in roughly 1 in 5 patients. It's not FDA-approved yet. Earliest possible approval is late 2027 or 2028.
Retatrutide is the first triple hormone receptor agonist to reach phase 3 clinical trials for obesity. It activates GLP-1, GIP, and glucagon receptors in a single molecule, producing the largest weight reductions reported for any anti-obesity peptide in clinical development. Phase 2 data published in the New England Journal of Medicine showed 24.2% mean weight loss at 48 weeks. Phase 3 topline data from December 2025 pushed that to 28.7% at 68 weeks, an average loss of 71.2 lbs. The drug is not yet approved. This article covers what the clinical evidence shows, where the risks are, and how retatrutide fits into the broader weight loss pipeline. For details on its mechanism, see How Retatrutide Targets Three Receptors at Once. For the pillar overview of retatrutide across all its applications, see Retatrutide and Liver Fat.
Key Takeaways
- Retatrutide is the next generation weight loss shot — the first drug that hits three hormone targets at once instead of one or two.
- In its first phase 3 trial, people lost 28.7% of their body weight over 68 weeks. That's about 71 pounds on average — the biggest number from any weight loss drug trial ever.
- Ozempic-type drugs handle hunger. Mounjaro adds blood sugar. Retatrutide adds a third job: telling your liver to burn stored fat.
- Liver fat dropped by up to 86% in less than a year. For fatty liver disease, which affects 1 in 4 adults, that's a bigger effect than anything else in development.
- The price is real side effects. About 1 in 5 people on the highest dose quit the trial because of them — more than twice the rate for approved weight loss drugs.
- A new side effect showed up: strange skin sensations (tingling, burning, pins-and-needles) in roughly 1 in 5 people. No one knows yet what's causing it.
- It's not FDA-approved. Seven more phase 3 trials report through 2026, and the earliest realistic approval date is late 2027 or 2028.
How Retatrutide Works
Retatrutide (LY3437943) activates three metabolic hormone receptors:
GLP-1 receptor: Suppresses appetite through hypothalamic signaling, slows gastric emptying, and enhances insulin secretion. This is the same target as semaglutide (Ozempic/Wegovy) and the GLP-1 component of tirzepatide (Mounjaro/Zepbound).
GIP receptor: Enhances the insulin response to meals, improves lipid metabolism, and may contribute to weight loss through mechanisms still under investigation. GIP receptor agonism is shared with tirzepatide.
Glucagon receptor: Increases hepatic fatty acid oxidation, stimulates energy expenditure, and reduces liver fat. This is the component unique to retatrutide. Glucagon normally raises blood sugar, but in combination with GLP-1 and GIP agonism, the glucose-raising effect is counterbalanced by enhanced insulin signaling.[3]
The triple agonist hypothesis holds that combining all three receptor targets in one molecule produces additive or synergistic metabolic benefits. The clinical data so far supports this: retatrutide produces larger weight reductions, greater liver fat clearance, and broader metabolic improvements than mono- or dual-agonist peptides in comparable trial designs.
Three Receptors, Three Jobs
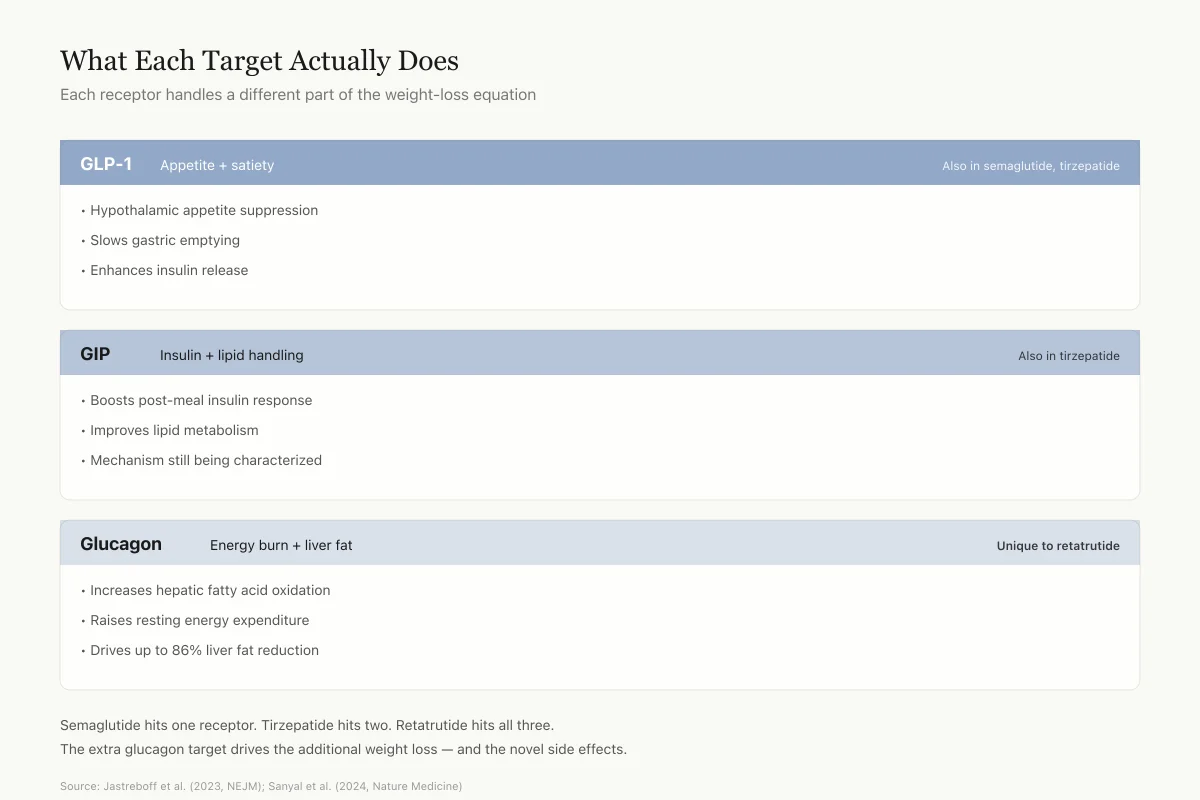
What Each Target Actually Does
Each receptor handles a different part of the weight-loss equation
- •Hypothalamic appetite suppression
- •Slows gastric emptying
- •Enhances insulin release
- •Boosts post-meal insulin response
- •Improves lipid metabolism
- •Mechanism still being characterized
- •Increases hepatic fatty acid oxidation
- •Raises resting energy expenditure
- •Drives up to 86% liver fat reduction
Semaglutide hits one receptor. Tirzepatide hits two. Retatrutide hits all three. The extra glucagon target is where the liver fat effect and the additional weight loss come from — and where the novel side effects likely come from too.
Source: Jastreboff et al. (2023, NEJM); Sanyal et al. (2024, Nature Medicine)
 View as image
View as imagePhase 2 Obesity Trial (NEJM, 2023)
Jastreboff et al. published the foundational retatrutide obesity data in the New England Journal of Medicine.[1]
Design: Phase 2, double-blind, randomized, placebo-controlled. 338 adults with BMI 30+ (or 27+ with a weight-related condition). 51.8% men. Participants were randomized to weekly subcutaneous retatrutide (1, 4, 8, or 12 mg) or placebo for 48 weeks.
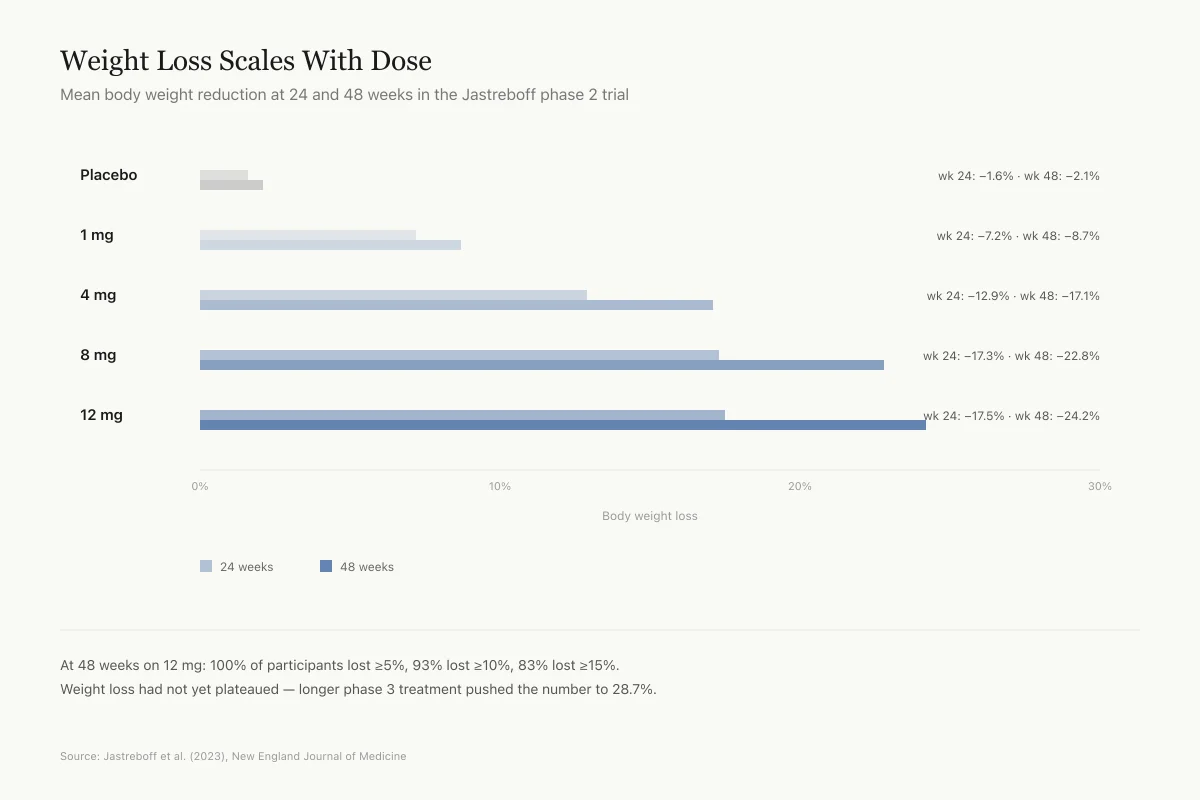
24-week results (primary endpoint):
- Placebo: -1.6%
- 1 mg: -7.2%
- 4 mg (combined): -12.9%
- 8 mg (combined): -17.3%
- 12 mg: -17.5%
48-week results:
- Placebo: -2.1%
- 1 mg: -8.7%
- 4 mg: -17.1%
- 8 mg: -22.8%
- 12 mg: -24.2%
At 48 weeks with the 12 mg dose, 100% of participants lost at least 5% of body weight, 93% lost at least 10%, and 83% lost at least 15%. Weight loss had not fully plateaued by week 48, suggesting further reduction with longer treatment.
Phase 2 Dose Response
Weight Loss Scales With Dose
Mean body weight reduction at 24 and 48 weeks in the Jastreboff phase 2 trial
At 48 weeks on 12 mg: 100% of participants lost at least 5% of body weight, 93% lost at least 10%, and 83% lost at least 15%. Weight loss had not yet plateaued — longer treatment in phase 3 pushed the number to 28.7%.
Source: Jastreboff et al. (2023), New England Journal of Medicine
 View as image
View as imageSafety: The most common adverse events were gastrointestinal (nausea, diarrhea, vomiting), dose-related, and mostly mild to moderate. Starting at 2 mg rather than 4 mg partially mitigated early GI symptoms. Dose-dependent heart rate increases peaked at 24 weeks and declined thereafter.
Phase 2 Type 2 Diabetes Trial (Lancet, 2023)
Rosenstock et al. evaluated retatrutide in people with type 2 diabetes in a parallel phase 2 program.[3]
The trial enrolled adults aged 18-75 with T2D, HbA1c 7.0-10.5%, and BMI 25-50. Retatrutide produced clinically meaningful improvements in glycemic control alongside robust weight reductions. HbA1c reductions were significant across dose groups, confirming that the triple agonist mechanism addresses both weight and blood sugar.
This matters because most people with severe obesity also have insulin resistance or type 2 diabetes. A drug that effectively treats both conditions simultaneously has obvious clinical advantages over treating each separately. The clinical trial results article provides deeper analysis of the dose-response data across both trials.
Phase 3: TRIUMPH-4 Results (December 2025)
In December 2025, Eli Lilly released topline results from TRIUMPH-4, the first completed phase 3 trial for retatrutide. The study enrolled adults with obesity or overweight who also had knee osteoarthritis.
Weight loss results at 68 weeks:
- Retatrutide 9 mg: -26.4% mean body weight loss
- Retatrutide 12 mg: -28.7% mean body weight loss (average 71.2 lbs)
- Placebo: not disclosed in topline data
These results exceeded the phase 2 data, which was expected given the longer treatment duration (68 vs. 48 weeks). At 28.7%, retatrutide produced the largest average weight reduction reported for any anti-obesity drug in a phase 3 trial.
Additional findings:
- Significant reduction in knee osteoarthritis pain scores
- Reduced non-HDL cholesterol, triglycerides, and hsCRP (cardiovascular risk markers)
- Systolic blood pressure reduced by 14.0 mmHg at the highest dose
Safety concerns:
- Discontinuation due to adverse events: 12.2% (9 mg), 18.2% (12 mg), 4.0% (placebo). Among participants with baseline BMI 35+, rates were lower: 8.8% and 12.1%.
- Nausea: 38.1% (9 mg), 43.2% (12 mg), 10.7% (placebo)
- Diarrhea: 34.7% (9 mg), 33.1% (12 mg), 13.4% (placebo)
- Dysesthesia (abnormal sensation): 8.8% (9 mg), 20.9% (12 mg), 0.7% (placebo). This is a new safety signal not prominent in phase 2 data. The events were generally mild and rarely led to discontinuation, but the dose-dependent pattern requires monitoring in ongoing trials.
These are topline results from a press release. Peer-reviewed publication with full data, including detailed subgroup analyses and quality-of-life measures, is pending. Seven additional TRIUMPH phase 3 readouts are expected in 2026, including studies on maintenance dosing strategies and specific patient populations.
Safety
ModerateThe dysesthesia signal is new and dose-dependent
Concern
Dysesthesia — abnormal skin sensations like tingling, burning, or pins-and-needles — appeared in 20.9% of the 12 mg arm versus 0.7% of placebo. It was not a prominent signal in phase 2. The dose-dependent pattern (8.8% at 9 mg, 20.9% at 12 mg) suggests a real drug effect, and the mechanism is not yet understood. Neither semaglutide nor tirzepatide produced this signal at meaningful rates.
What the research says
Events were generally mild and rarely led to discontinuation. Whether this resolves on continued treatment, whether it signals any underlying nerve effect, and whether long-term dosing makes it worse — all open questions. The remaining TRIUMPH trials will provide more data.
Particularly relevant for: Anyone considering the 12 mg dose should know about this before starting; people with existing neuropathy or unexplained nerve symptoms especially
What to do
Report new or worsening skin sensations to your prescriber. If it's severe or persistent, dose reduction may be appropriate. Monitor across the full TRIUMPH program readouts before treating this as a settled safety profile.
TRIUMPH-4 topline safety data (Eli Lilly, 2025)
Pooled Evidence: What the Meta-Analysis Shows
Abdrabou et al. (2025) published a systematic review and meta-analysis of retatrutide across three randomized controlled trials encompassing 878 patients.[4]
Pooled results showed retatrutide significantly reduced:
- Body weight: mean difference -14.33% (P < 0.00001)
- BMI: -5.38 (P < 0.00001)
- Waist circumference: -10.51 cm (P < 0.00001)
- Fasting plasma glucose: -23.51 mg/dL (P < 0.00001)
- HbA1c: -0.91% (P < 0.00001)
- Blood pressure: statistically significant reductions (P < 0.00001)
The meta-analysis confirmed a dose-dependent relationship, with 12 mg producing maximum reductions across all measured outcomes. The safety profile was consistent across trials, with GI events being the primary concern.
How It Compares
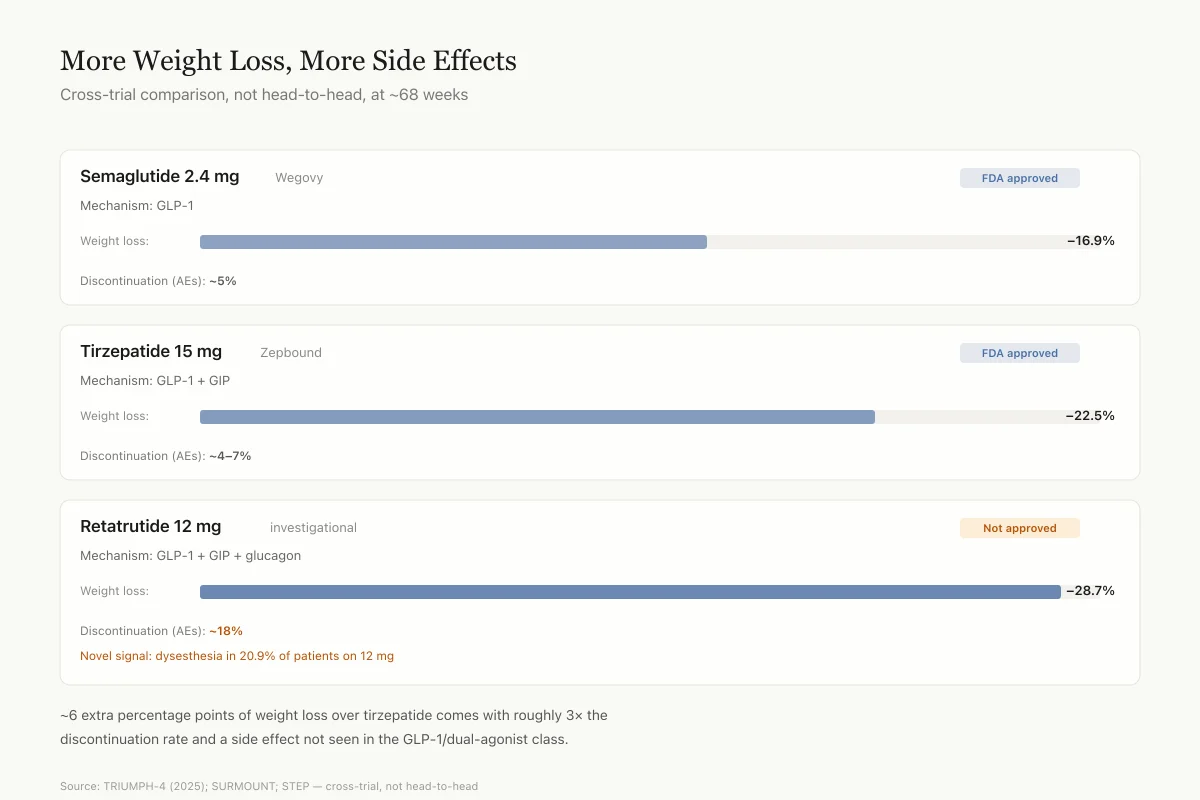
No head-to-head trials have been conducted between retatrutide and its competitors. Cross-trial comparisons are imperfect due to differences in patient populations, trial duration, and endpoints. With that caveat, the approximate weight loss landscape at comparable timepoints:
| Drug | Mechanism | Max Weight Loss | Timepoint |
|---|---|---|---|
| Retatrutide 12 mg | GLP-1 + GIP + glucagon | 28.7% | 68 weeks (Phase 3) |
| Tirzepatide 15 mg | GLP-1 + GIP | ~22.5% | 72 weeks (Phase 3) |
| Semaglutide 2.4 mg | GLP-1 | ~16.9% | 68 weeks (Phase 3) |
Retatrutide's additional weight loss over tirzepatide is roughly 6 percentage points. Whether this incremental benefit justifies the additional safety burden (higher discontinuation rates, the dysesthesia signal) is a clinical question that cannot be answered from current data alone. The retatrutide vs. tirzepatide vs. semaglutide comparison article covers this in more detail.
A Bayesian network meta-analysis of 19 randomized controlled trials (29,506 adults) found that retatrutide and dual agonists achieved equivalent mean weight loss (-11.0 kg), but retatrutide excelled at achieving the deepest weight loss thresholds (15%+ body weight reduction). This suggests the triple mechanism may particularly benefit patients who need the largest absolute weight reductions.
The safety comparison is equally important. Tirzepatide's discontinuation rate due to adverse events in SURMOUNT trials was approximately 4-7%, substantially lower than retatrutide's 12-18%. Semaglutide's rates are similar to tirzepatide's. The additional efficacy of retatrutide comes with a measurably higher tolerability cost, and the dysesthesia signal has no parallel in the GLP-1 or dual agonist class.
Cross-Trial Comparison
More Weight Loss, More Side Effects
Not head-to-head, but an apples-to-apples look at the top three
Mechanism: GLP-1
Mechanism: GLP-1 + GIP
Mechanism: GLP-1 + GIP + glucagon
Retatrutide's ~6 extra percentage points of weight loss over tirzepatide comes with roughly 3× the discontinuation rate and a side effect (dysesthesia) not seen in the GLP-1/dual-agonist class. Whether that tradeoff is acceptable is an individual clinical decision once the drug is available.
Source: TRIUMPH-4 topline (Eli Lilly, 2025); SURMOUNT trials (Jastreboff 2022); STEP trials (Wilding 2021) — cross-trial, not head-to-head
 View as image
View as imageThe Liver Bonus
Unlike single or dual agonists, retatrutide produces dramatic liver fat reduction. In the MASLD substudy, Sanyal et al. (2024) reported up to 86% relative liver fat reduction at 48 weeks, with 93% of participants on 12 mg achieving normal liver fat levels.[2] This effect appears driven by the glucagon receptor component stimulating hepatic fatty acid oxidation, as evidenced by 2-3 fold increases in beta-hydroxybutyrate levels. For a full analysis of the liver data, see Retatrutide and Liver Fibrosis: Triple Agonist Data.
What Remains Unknown
Long-term safety beyond 68 weeks: The longest published data is 48 weeks (phase 2). TRIUMPH-4 extends to 68 weeks. What happens with years of treatment is unknown. The dysesthesia signal warrants particular long-term monitoring.
Weight regain after stopping: No published data exists on what happens to weight when retatrutide is discontinued. Based on experience with GLP-1 agonists, substantial regain is expected.
Cardiovascular outcomes: Retatrutide reduces cardiovascular risk markers (blood pressure, lipids, hsCRP), but no dedicated cardiovascular outcomes trial has been completed. This data is critical given the heart rate elevation seen in trials.
Muscle mass preservation: At 28.7% weight loss, muscle loss is a serious concern. In typical weight loss, roughly 25-40% of lost weight comes from lean mass rather than fat. A body composition substudy of retatrutide in people with type 2 diabetes has been published (Lancet Diabetes Endocrinol, 2025), but comprehensive lean mass data from the phase 3 obesity population is not yet available. Whether the glucagon component's effect on protein metabolism helps or hinders muscle preservation is an open question.
Cost and access: If approved, retatrutide's pricing and insurance coverage will determine real-world impact. Current GLP-1 agonists cost $800-1,300 per month at list price, and coverage remains inconsistent. A triple agonist with premium pricing could face even greater access barriers.
Approval timeline: Retatrutide is not FDA-approved. Seven TRIUMPH phase 3 trials are expected to report in 2026. Regulatory filing timelines have not been announced. For the latest on when retatrutide may be available, see our timeline article.
The Bottom Line
Retatrutide is the most potent anti-obesity peptide in clinical development, producing up to 28.7% body weight loss in phase 3 data. Its triple receptor mechanism (GLP-1 + GIP + glucagon) generates larger weight reductions and liver fat clearance than dual or single agonists. The tradeoff is higher discontinuation rates (up to 18.2%) and a new dysesthesia signal not seen with other incretin-based drugs. Phase 3 data is still emerging, with seven additional TRIUMPH trials expected to report in 2026. The drug is not approved anywhere in the world as of March 2026.
Sources & References
- 1RPEP-07002·Jastreboff, Ania M et al. (2023). “Triple-Hormone-Receptor Agonist Retatrutide for Obesity - A Phase 2 Trial..” The New England journal of medicine.Study breakdown →PubMed →↩
- 2RPEP-09206·Sanyal, Arun J et al. (2024). “Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial..” Nature medicine.Study breakdown →PubMed →↩
- 3RPEP-07323·Rosenstock, Julio et al. (2023). “Retatrutide Phase 2 Trial: The Triple-Receptor Agonist Cut HbA1c by 2% and Weight by 17% in Type 2 Diabetes.” Lancet (London.Study breakdown →PubMed →↩
- 4RPEP-09740·Abdrabou Abouelmagd, Alaa et al. (2025). “Retatrutide: The Triple Agonist Peptide Targeting GLP-1, GIP, and Glucagon Receptors.” Proceedings (Baylor University. Medical Center).Study breakdown →PubMed →↩