Caloric Intake on GLP-1 Therapy: How Low Is Too Low?
GLP-1 Nutrition and Diet
16-39% caloric reduction on GLP-1 drugs
GLP-1 receptor agonists reduce spontaneous food intake by 16-39%, creating caloric deficits that drive weight loss but also raise the risk of nutritional deficiencies, muscle loss, and metabolic adaptation when intake drops too low.
Dietary intake review, Obesity Reviews, 2024
Dietary intake review, Obesity Reviews, 2024
If you only read one thing
Most adults should not drop below 1,200 calories a day (women) or 1,500 calories a day (men) while on semaglutide or tirzepatide. Below that, it gets hard to hit your protein and vitamin needs from food alone. GLP-1 drugs kill hunger so effectively that many people eat too little without noticing — and about 1 in 4 develop a nutritional deficiency within the first year. Aim for steady weight loss of 0.5-1% per week, hit your protein target (around 100 grams a day for most adults), and lift weights twice a week to protect your muscle.
GLP-1 receptor agonists like semaglutide and tirzepatide work in part by reducing appetite. That is both their mechanism of action and their potential problem. When appetite suppression is too effective, patients eat too little, and "too little" has measurable consequences: nutritional deficiencies, accelerated muscle loss, metabolic adaptation, and in rare cases, clinical malnutrition. A narrative review in Obesity Reviews found that GLP-1 and dual GIP/GLP-1 receptor agonists reduce caloric intake by 16-39% across clinical studies. For someone eating 2,000 calories per day, that is a reduction of 320-780 calories, potentially dropping intake below the thresholds where essential nutrients become difficult to obtain from food alone.
This article examines what the evidence says about minimum caloric intake during GLP-1 therapy, the consequences of going too low, and the protein and nutrition strategies that the clinical data supports. For the specific vitamin and mineral deficiencies that emerge during GLP-1 therapy, see the pillar article.
Key Takeaways
- GLP-1 drugs cut how much people eat by 16–39% — often without them noticing.
- About 1 in 4 GLP-1 patients develops a nutritional deficiency in their first year.
- Eating even less than the drug already cuts doesn't speed up fat loss — it speeds up muscle loss.
- Most women shouldn't drop below 1,200 calories a day on these drugs — most men not below 1,800.
- About 25–30% of weight lost on these drugs comes from muscle, not fat.
- The simplest fix: hit a protein target around 100 grams a day and lift weights twice a week.
- GLP-1 drugs already create a calorie deficit on their own — stacking extreme restriction turns healthy loss into starvation.
How Much Less Do People Actually Eat?
The caloric reduction from GLP-1 therapy has been quantified in controlled studies.
Gibbons et al. (2021) conducted one of the most rigorous assessments, measuring the effects of oral semaglutide on energy intake using standardized ad libitum meals. Patients on semaglutide reduced their total daily energy intake by approximately 24% (about 530 kcal/day) over 20 weeks. The reduction was driven primarily by decreased appetite and increased satiety rather than food aversion or nausea.[1]
Gabe et al. (2024) confirmed these findings in a subsequent study of oral semaglutide's effects on energy intake, appetite, control of eating, and gastric emptying. The appetite suppression was consistent across meal types and times of day, suggesting a central mechanism rather than a gastric motility effect alone.[2]
Basolo et al. (2025) measured the 24-hour energy metabolism effects of 6 months of liraglutide treatment, providing detailed data on both intake reduction and metabolic rate changes that accompany prolonged GLP-1 therapy.[3]
The 16-39% range across studies reflects variation in the specific drug, dose, patient population, and measurement method. Higher-dose semaglutide (2.4 mg weekly) and tirzepatide tend toward the higher end of caloric reduction.
The Minimum Intake Thresholds
No GLP-1-specific clinical guideline defines a universal minimum caloric intake. But the general nutrition science is clear on where deficiency risk begins.
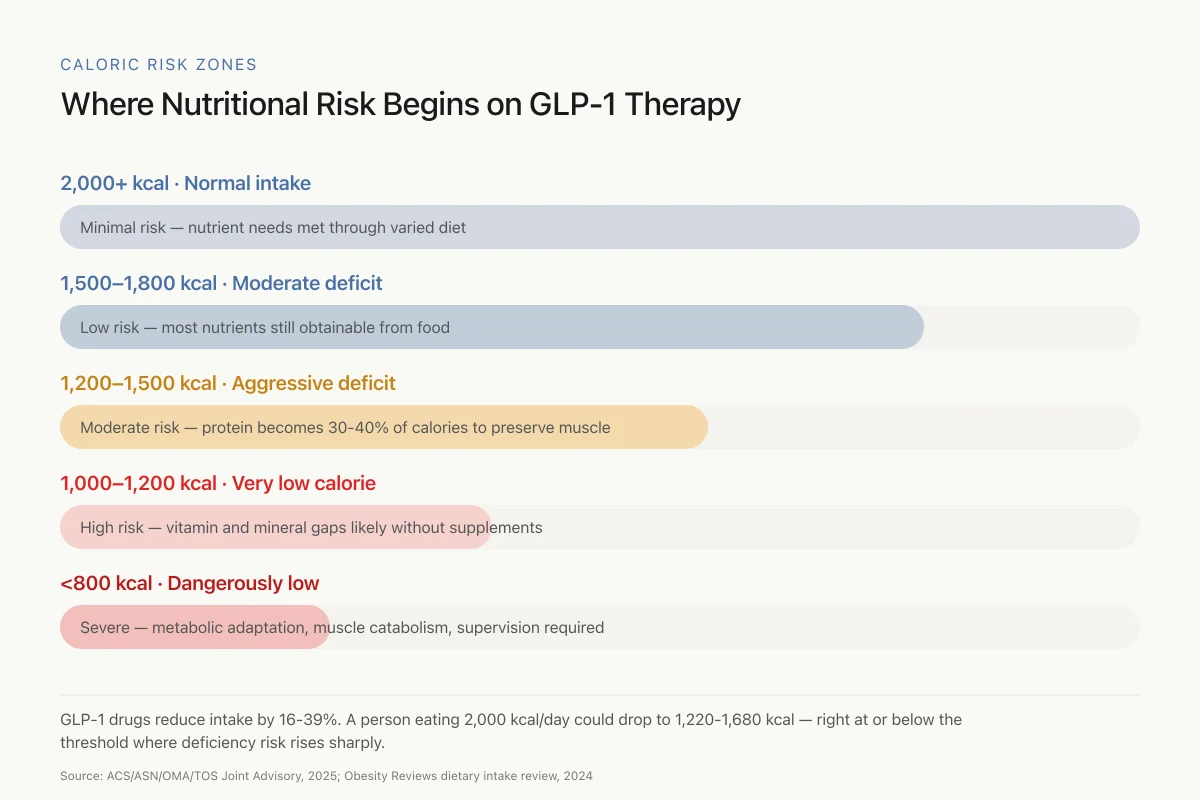
Below 1,200 kcal/day (women) and 1,800 kcal/day (men): At these levels, meeting recommended daily intakes of essential vitamins and minerals through food alone becomes increasingly unlikely. Iron, calcium, magnesium, zinc, and vitamins A, D, E, K, B1, B12, and C are the nutrients most at risk. A joint advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and the Obesity Society specifically flagged these thresholds in the context of GLP-1 therapy.
Below 1,000 kcal/day: This level is classified as a very-low-calorie diet (VLCD) and carries risks of gallstone formation, cardiac arrhythmias (from electrolyte imbalances), hair loss, and muscle catabolism. VLCDs require medical supervision even without GLP-1 therapy. On GLP-1 drugs, some patients spontaneously reach VLCD-level intake without intending to, simply because appetite is so effectively suppressed.
Below 800 kcal/day: Associated with adaptive thermogenesis (metabolic rate drops disproportionately to weight lost), increased cortisol, thyroid hormone suppression, and significant lean mass loss. Daou et al. (2025) described a case combining very-low-calorie diet with tirzepatide and bariatric surgery, illustrating the extreme end of the caloric deficit spectrum that some clinical protocols employ under strict supervision.[4]
Caloric Risk Zones
Where Nutritional Risk Begins on GLP-1 Therapy
GLP-1 drugs reduce intake by 16-39%. A person eating 2,000 kcal/day could drop to 1,220-1,680 kcal — right at or below the threshold where deficiency risk rises sharply.
Source: ACS/ASN/OMA/TOS Joint Advisory, 2025; Obesity Reviews dietary intake review, 2024
 View as image
View as imageThe Lean Mass Problem
Weight loss from any cause, whether dietary restriction, surgery, or GLP-1 therapy, involves some loss of lean mass (muscle, bone, organ tissue) alongside fat loss. The ratio matters enormously.
Bhandarkar et al. (2025) reviewed the effect of GLP-1 receptor agonists on body composition, finding that approximately 25-30% of total weight lost with GLP-1 drugs is lean mass, with 70-75% being fat mass.[5] This ratio is similar to what is observed with dietary restriction alone, suggesting the lean mass loss is a consequence of caloric deficit rather than a direct pharmacological effect on muscle.
Rodriguez et al. (2024) examined body composition changes with semaglutide in adults with obesity and Type 2 diabetes, confirming that semaglutide produced meaningful reductions in visceral and subcutaneous fat alongside modest lean mass decreases.[6]
Choi et al. (2024) provided a more nuanced perspective, demonstrating that semaglutide-induced weight loss actually improved mitochondrial energy efficiency in skeletal muscle, suggesting that the remaining muscle tissue may function better even as total lean mass decreases.[7]
Chun et al. (2025) assessed weight loss and body composition after compounded semaglutide in a real-world setting, providing data from outside the controlled trial environment where dietary compliance and monitoring are less rigorous.[8]
When lean mass loss becomes dangerous
Stefanakis et al. (2024) published a comprehensive analysis of the impact of weight loss on fat-free mass, muscle, bone, and hematopoiesis health, directly addressing the implications for GLP-1 therapy. The critical finding: lean mass loss becomes clinically significant when it drops below the threshold for functional independence, particularly in older adults.[9]
Jadvani et al. (2025) reported a case of rhabdomyolysis (acute muscle breakdown) linked to semaglutide use, an extreme but instructive example of what can happen when severe caloric restriction and muscle stress combine.[10] While rhabdomyolysis with GLP-1 drugs is rare, it represents the far end of a spectrum that begins with gradual, clinically silent muscle loss.
For a deeper examination of the sarcopenia risk in older adults on GLP-1s, see the dedicated article.
The Protein Priority
The single most evidence-supported strategy for preserving lean mass during GLP-1 weight loss is adequate protein intake. The current recommendation from multiple obesity medicine guidelines is 1.2-1.6 g of protein per kilogram of ideal body weight per day, combined with resistance training 2-3 times weekly.
This protein target is challenging for patients on GLP-1 drugs because appetite suppression affects protein-containing foods as much as other foods, and protein is the most satiating macronutrient, meaning it is often the first thing patients reduce when appetite drops. When total caloric intake falls below 1,200-1,500 calories, meeting 1.2 g/kg of protein requires that protein comprise 30-40% of total calories, a much higher proportion than most people naturally consume.
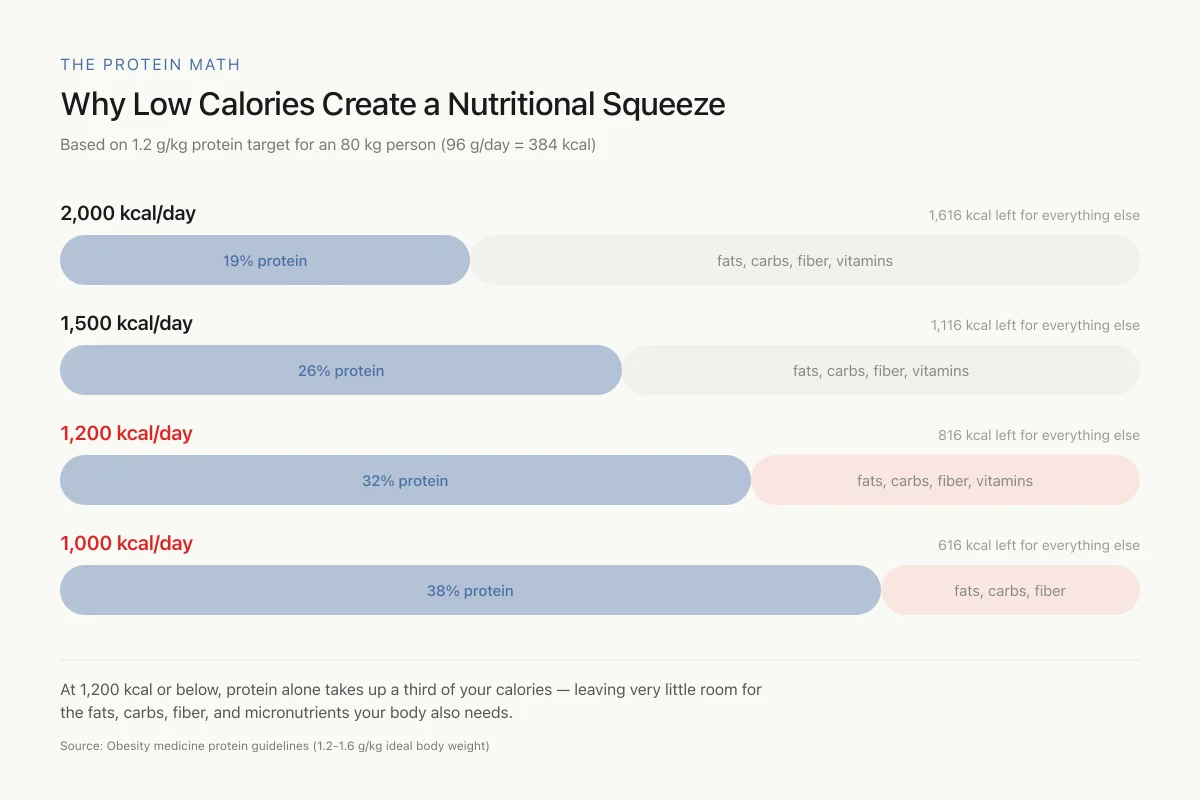
The Protein Math
Why Low Calories Create a Nutritional Squeeze
Based on 1.2 g/kg protein target for an 80 kg person (96 g/day = 384 kcal)
At 1,200 kcal or below, protein alone takes up a third of your calories — leaving very little room for the fats, carbs, fiber, and micronutrients your body also needs. This is why caloric intake below 1,200 creates a nutritional trap.
Source: Obesity medicine protein guidelines (1.2-1.6 g/kg ideal body weight)
 View as image
View as imagePractical implications:
- A 70 kg person needs 84-112 g of protein daily (at 1.2-1.6 g/kg)
- At 1,200 calories/day, that protein accounts for 336-448 calories (28-37% of total intake)
- At 1,000 calories/day, protein would need to be 34-45% of intake, leaving minimal room for carbohydrates, fats, fiber, and micronutrients
This arithmetic shows why caloric intake below 1,200 creates a nutritional squeeze: protein needs are non-negotiable for muscle preservation, but meeting them at very low caloric intakes crowds out other essential nutrients.
When Patients Are Eating Too Little: Warning Signs
The challenge with GLP-1-mediated appetite suppression is that patients may not recognize they are eating too little. Unlike intentional caloric restriction, where hunger serves as feedback, GLP-1 drugs eliminate the hunger signal. Patients can operate at significant caloric deficits without feeling hungry or deprived.
Clinical indicators that caloric intake has dropped too low:
- Rapid weight loss exceeding 1% of body weight per week after the first month
- Hair loss (telogen effluvium, typically appearing 3-6 months after onset of severe deficit)
- Persistent fatigue unrelated to medication side effects
- Dizziness or orthostatic hypotension from electrolyte imbalances
- Laboratory findings: low albumin, low prealbumin, anemia, electrolyte abnormalities
- Amenorrhea in premenopausal women (indicating energy availability below the threshold for reproductive function)
- Progressive weakness or declining functional capacity despite adequate physical activity
Safety
ModerateHunger cues stop working — but the risk doesn't
Concern
GLP-1 drugs suppress hunger so effectively that patients can slide into very-low-calorie territory without feeling deprived. The usual early warning — being hungry — is gone. By the time symptoms like hair loss, fatigue, or dizziness appear, a patient has often been under-eating for months.
What the research says
Track caloric intake explicitly for the first 3-6 months of therapy — at least a rough estimate from an app or food log. Don't rely on hunger as a signal. Get baseline labs (iron, B12, vitamin D, albumin, electrolytes) and recheck at 6 and 12 months.
Particularly relevant for: Anyone on semaglutide, tirzepatide, or liraglutide — particularly higher doses and older adults
What to do
If weight loss exceeds 1% of body weight per week after the first month, slow the pace. Add calories deliberately. Check with your prescriber before assuming 'faster is better.'
ACS/ASN/OMA/TOS Joint Advisory (2025); observational cohort data on 460,000+ GLP-1 patients
What the Nutrition Guidelines Recommend
The 2025 joint advisory from major obesity and nutrition societies provides the most comprehensive framework for nutrition during GLP-1 therapy:
- Minimum caloric floor: No less than 1,200 kcal/day for women or 1,500 kcal/day for men without medical supervision
- Protein target: 1.2-1.6 g/kg ideal body weight daily, distributed across 3+ meals
- Resistance training: 2-3 sessions per week to provide the mechanical stimulus for muscle preservation
- Micronutrient monitoring: Baseline and periodic assessment of iron, calcium, vitamin D, B12, and other nutrients of concern
- Registered dietitian involvement: Patients working with dietitians during GLP-1 therapy have better nutritional outcomes
- Rate of weight loss: Aim for 0.5-1% of body weight per week after initial rapid loss phase
These recommendations apply across all GLP-1 receptor agonists, though the more potent drugs (high-dose semaglutide, tirzepatide) require more aggressive nutritional attention because they produce greater caloric reduction.
The Dose-Response Caloric Problem
Higher GLP-1 doses produce more appetite suppression, more weight loss, and more caloric reduction. This creates a paradox: the doses that produce the best weight loss outcomes also create the highest nutritional risk.
For semaglutide, the weight management dose (2.4 mg weekly) produces approximately twice the caloric reduction of the diabetes dose (1.0 mg weekly). For tirzepatide, the highest dose (15 mg weekly) produces substantially more appetite suppression than the starting dose (2.5 mg weekly).
Dose titration is designed to mitigate this problem by gradually increasing appetite suppression. But the titration schedule was designed for tolerability (reducing nausea and GI side effects), not for nutritional adequacy. A patient who tolerates 2.4 mg semaglutide without nausea may still be eating too few calories to meet their nutritional needs.
What the Research Does Not Yet Answer
Optimal caloric floor for GLP-1 patients specifically. Current minimum intake recommendations are adapted from general weight management guidelines, not derived from GLP-1-specific research. Whether GLP-1 drugs alter nutrient absorption, metabolism, or requirements in ways that change the minimum intake threshold is unknown.
Long-term lean mass trajectories. Most body composition data comes from trials lasting 52-72 weeks. Whether lean mass stabilizes, continues declining, or partially recovers during multi-year GLP-1 therapy has not been characterized.
Individual variation. The 16-39% caloric reduction range is an average. Some patients reduce intake by 10%, others by 50%+. Predicting who will develop dangerously low intake is not currently possible.
Interaction with how GLP-1 drugs change food relationships. Some patients report food aversion rather than simple appetite reduction. Whether food aversion leads to greater nutritional risk than appetite suppression alone has not been studied.
The Bottom Line
GLP-1 receptor agonists reduce caloric intake by 16-39%, creating the energy deficit that drives weight loss. Below 1,200 kcal/day for women and 1,800 kcal/day for men, meeting essential nutrient requirements from food alone becomes increasingly difficult, and 22% of patients develop nutritional deficiencies within 12 months. Approximately 25-30% of weight lost is lean mass, driven by caloric deficit rather than a direct drug effect on muscle. The evidence-based mitigation strategy is protein intake of 1.2-1.6 g/kg daily combined with resistance training, but meeting protein targets becomes arithmetically challenging when total caloric intake drops too low. Nutrition monitoring and dietitian involvement are recommended for all patients on GLP-1 therapy.
Sources & References
- 1RPEP-05404·Gibbons, Catherine et al. (2021). “Oral Semaglutide Cuts Daily Food Intake by 39% and Improves Eating Control.” Diabetes.Study breakdown →PubMed →↩
- 2RPEP-08228·Gabe, Maria Buur Nordskov et al. (2024). “Effect of oral semaglutide on energy intake, appetite, control of eating and gastric emptying in adults living with obesity: A randomized controlled trial..” Diabetes.Study breakdown →PubMed →↩
- 3RPEP-10109·Basolo, Alessio et al. (2025). “Liraglutide Causes Weight Loss Primarily From Fat While Shifting the Body to Burn More Fat for Fuel.” Journal of endocrinological investigation.Study breakdown →PubMed →↩
- 4RPEP-10618·Daou, Carla et al. (2025). “Very-low-calorie-diet, tirzepatide, and bariatric surgery: a multidisciplinary success in super-super obesity..” Journal of surgical case reports.Study breakdown →PubMed →↩
- 5RPEP-10144·Bhandarkar, Akhila et al. (2025). “Effect of GLP-1 receptor agonists on body composition..” Current opinion in endocrinology.Study breakdown →PubMed →↩
- 6RPEP-09164·Rodríguez Jiménez, Beatriz et al. (2024). “Semaglutide Reduces Body Fat in Obese Diabetes Patients Regardless of Formulation.” Frontiers in endocrinology.Study breakdown →PubMed →↩
- 7RPEP-08004·Choi, Ran Hee et al. (2024). “Semaglutide-induced weight loss improves mitochondrial energy efficiency in skeletal muscle..” bioRxiv : the preprint server for biology.Study breakdown →PubMed →↩
- 8RPEP-10499·Chun, Elizabeth et al. (2025). “Compounded Semaglutide Produced Meaningful Weight Loss and Improved Body Composition in a Real-World Setting.” Diabetes.Study breakdown →PubMed →↩
- 9RPEP-09318·Stefanakis, Konstantinos et al. (2024). “Weight Loss Drugs Risk Muscle and Bone Loss: The Case for Myostatin Inhibitors as Combination Therapy.” Metabolism: clinical and experimental.Study breakdown →PubMed →↩
- 10RPEP-11551·Jadvani, Rutvikkumar et al. (2025). “From weight loss to muscle loss: rhabdomyolysis linked to semaglutide..” Clinical kidney journal.Study breakdown →PubMed →↩